What the War on Chlorine Dioxide Reveals About Medicine
For over a century, remarkable therapies have been suppressed to maintain a medical monopoly at the expense of humanity
Story at a Glance:
Modern medicine is built around costly, narrowly approved drugs that treat (but rarely cure) specific disease franchises, with regulatory approval correlating more strongly with money spent than with real therapeutic value.
To enforce this, for over a century the same institutions, backed by vast fortunes, have repeatedly sidelined broader or cheaper therapies that threatened those franchises.
The same playbook is used again and again—once a therapy threatens a market, claims of “no evidence” or doctored research amplified by the media will allow regulators to clamp down on the “dangerous and unproven” therapy until it becomes forgotten to history.
In this article, I will illustrate how the exact same playbook was used again and again on numerous transformative medical discoveries endorsed by leading physicians of the era, resulting in nearly every one (e.g., UVBI and numerous cancer treatments) becoming largely forgotten despite immense evidence behind them.
This same playbook was used throughout COVID-19 to eliminate the off-patent therapies that threatened the boondoggle. One of these, chlorine dioxide, was not only repeatedly shown to eliminate COVID outbreaks, but also to do the same with malaria, where it likewise was banned.
Pierre Kory and Jenna McCarthy’s recent book The War on Chlorine Dioxide provides a critical body of evidence that chlorine dioxide has treated a myriad of challenging conditions, and that each time it did, a robust censorship apparatus erased those discoveries and retaliated against the discovers—providing a poignant illustration of the medical monopoly in action.
While medicine has produced remarkable and life-changing results for a variety of challenging conditions, the present reality of our medical system is that:
• Large amounts of research dollars are collected each year to seek out solutions for incurable diseases creating immense suffering for many patients with “incurable” conditions.
• Since many diseases lack satisfactory treatments, patients and health care systems begrudgingly accept paying for and using the unsatisfactory treatments that are available.
• When medicine is ultimately unable to address a condition patients have, this is justified under the logic “we tried everything we had and nothing more could be done” (e.g., for a hospitalized patient, or more recently, for a disabled patient being funneled into medically assisted dying).
Our medical system, in turn, is structured so that:
• For a therapy to enter regular use (and particularly for it to be paid for) it must secure a regulatory approval.
• Regulatory approvals require a body of preclinical science (which if often the results of years of public research dollars), a mechanistic basis (that typically draws upon those studies), costly large randomized controlled trials and effective regulatory lobbying (all of which results in drugs now typically costing 1-2 billion dollars to bring to market1,2,3). However, while there is a strong correlation between spending money to secure an approval and receiving it, a much weaker correlation exists between the intrinsic value of a treatment and its approval (resulting in many unsafe drugs being approved that provide negligible benefits).
• Once a drug is brought to market, payers will pay vast sums of money for the treatment, in part to cover the cost of bringing it to market.
• The regulatory approval process typically rewards drugs having a specific mechanism for a specific disease. Because of this, each disease becomes a lucrative franchise that is reserved for a limited number of pharmaceuticals (which utilize a limited number of approved mechanisms) that in most cases provide an unsatisfactory treatment, making it possible to reuse the franchise in the future with a new class of drugs once the patents on the original ones run out.
Note: “franchise” is a term routinely used in the pharmaceutical industry.
• While the rules for getting an FDA approval are quite strict, once approved, the rules for using an approved drug for something else are quite lax, and as such, pharmaceutical drugs are routinely used to treat conditions they lack evidence for treating.
If you take a step back, this entire paradigm relies upon two things:
- The belief that a substance, by virtue of being labeled as a pharmaceutical (through regulatory approval), is “real medicine” that works (and must have extensive credible evidence behind it).
- For each of these disease franchises to remain incurable so that an endless funnel of money can go into bringing us closer to a cure (which occasionally new pharmaceuticals accomplish, but typically do not).
Many hence find the existing paradigm extremely frustrating, in part because of how much money it sucks up (which has now hit the point socialist states are pursuing medically assisted dying to balance their budgets), and in part because of how much the people with these “incurable” diseases suffer year after year after year.
A History of Medicine
Understanding where the current paradigm comes from requires understanding the history of medicine.
In the earliest recorded history, disease was widely attributed to supernatural causes (e.g., angry gods, demons, ancestral spirits, curses, or soul loss) and medicine typically involved shamans, priests, or medicine men using rituals, incantations, charms, amulets, sacrifices, and exorcisms, often combined with herbal remedies or basic surgery (e.g., trepanation to release evil energy from the head).
Note: while these supernatural approaches have still been largely discarded, some are still utilized by spiritual healers and indigenous traditions (e.g., Native American and Amazonian shamans) and every now and then, I hear of someone treating a fairly challenging illness with one.
Around the time of Christ (400 BC – 100 AD) a new perspective entered the world that led to medical systems across numerous major civilizations concluding illness resulted from innate qualities within the body being out of balance or obstructed (e.g., the four humors, yin and yang, the five elements, the doshas etc) and hence that healing arose from harmoniously rebalancing them. Due to the success of this approach, it supplemented and then gradually displaced old approaches like human sacrifice.
Note: certain points of evidence suggest the “balance” school of medicine originated from a much older society that predated recorded history (e.g., it’s referenced in the opening of the original text of Chinese of medicine and Graham Hancock has built an extensive case an older advanced civilization was mostly but not completely erased by a planetary disaster).
After the classical balance systems became established, they remained the dominant medical framework for well over a thousand years. In Rome, Galen (129-216 AD) then refined Greek humoral theory with extensive anatomy and physiology derived from animal dissections and experiments (human ones were illegal), causing the synthesis of the four humors with detailed organ function and bodily structure to become the authoritative medical model across Europe and then the Islamic world.
The Renaissance (roughly 1300–1600) and the Scientific Revolution that overlapped and followed it (roughly 1500–1700) produced major anatomical and physiological discoveries (most notably William Harvey’s 1628 demonstration that blood circulates in a closed circuit pumped by the heart) as well as philosophical shifts such as Descartes’ separation of mind (or soul) from body. Together these developments encouraged a new view of the body as a mechanical structure governed by physical laws and amenable to external analysis and intervention.
This gave birth to “heroic medicine” which used invasive methods, mineral remedies and toxic remedies (e.g. mercury, opium and antimony) to powerfully shift the body in the belief that would achieve health (with this school of medicine eventually coming to be known by many as “allopathy,” after the founder of homeopathy in 1810 critically coined this term to denote that this system worked by forcefully producing effects opposite to the symptoms of the disease).
Between the 1850s-1880s, advances in germ theory (Pasteur and Koch), cellular pathology (Virchow), controlled laboratory methods, and clinical observation shifted the understanding of disease toward specific, measurable causes such as microorganisms, cellular damage, chemical imbalances, and structural failures. The body was hence increasingly viewed as a complex biological machine that could be diagnosed and fixed through targeted interventions and in the early 1900s, this mechanistic approach had become the prevailing paradigm in Western medicine, after which it spread globally.
However, since allopathy had major shortcomings (e.g., it failed to treat many diseases, its remedies—particularly mercury and early vaccines like smallpox—created a horrendous wave of illnesses never seen before, and patients often died from allopathic methods), in the 1800s a variety of other medical schools emerged that gradually outcompeted allopathic medicine (homeopathy, osteopathy, “the eclectic” naturopathic school of medicine and to a lesser extent chiropractic—with doctors at the time often also being licensed in many of these schools).
Medical Monopolization
The American Medical Association, founded in 1847 partly to counter the newly established American Institute of Homeopathy, for decades remained relatively weak in membership and finances (as most MDs in the country did not wish to join that and homeopaths were far more prosperous due to them being preferred by the wealthy and most educated). However, two developments changed that trajectory.
First, internal reorganization of the AMA itself. In 1899 George H. Simmons became general manager (and later editor of the AMA’s widely read medical journal JAMA). Under Simmons and his successor Morris Fishbein (editor roughly 1924–1950), the association professionalized its operations, expanded membership dramatically, and created revenue streams tied to pharmaceutical advertising. The AMA Council on Pharmacy and Chemistry (1905) introduced a “Seal of Acceptance” program: companies disclosed ingredients and limited certain claims in exchange for the right to advertise in AMA publications.
Note: a friend knew Morris Fishbein’s secretary and shared with me the secretary witnessed highly unethical behavior from him consistent with his unscrupulous behaviors highlighted throughout this article.
Advertising revenue (according to the most commonly cited source) rose from roughly $34,000 in 1899 to $150,000 by 1909, while membership grew from about 8,000 to over 70,000. Critics at the time called the arrangement commercially self-serving but the AMA nevertheless gained resources and visibility.
Note: in many later accounts of the events, the AMA’s activities were characterized as monopolistic blackmail (with the AMA having a lengthy conflict with the founder of Abbott Laboratories), and while that seems likely given the AMA’s other activities, I have not located any sources from the time that substantiated overt blackmail occurred.
Likewise, the AMA had earlier used a “consultation clause” in its code of ethics that forbade members from associating with homeopaths (or other “irregulars”), with expulsion from local societies sometimes resulting in loss of licensure. Even after the clause was formally removed in 1901, homeopaths could join only by renouncing homeopathy in practice.
Second, there was a concerted push for higher educational and licensing standards. The AMA’s Council on Medical Education (established 1904) began rating schools. In 1910 the Carnegie Foundation published Abraham Flexner’s “Medical Education in the United States and Canada.” Flexner, working with input from AMA reformers (including close consultation with Nathan Colwell of the AMA Council and correspondence that treated the report as “ammunition” for the AMA while publicly distancing the collaboration), harshly criticized proprietary, under-resourced, and most sectarian schools—including the majority of the roughly 20–22 homeopathic colleges then operating—for inadequate laboratories, weak science prerequisites, and commercial incentives. State licensing boards increasingly aligned with these ratings. The result was rapid closure or conversion of many competing schools; by the 1930s the number of U.S. medical schools had fallen sharply (with Women’s and Black medical colleges disproportionately affected), homeopathic schools had dwindled to two by 1923, and the remaining institutions were almost entirely scientific and allopathic in orientation.
Note: a case can be made Flexner did this not to monopolize medicine, but simply to address poor standards in medical schools across the country, but many of his “standards” were based upon an allopathic worldview that placed a much greater weight on subjects like anatomy than homeopathic medical schools (where a precise knowledge of anatomy was not necessary to practice the discipline). That said, from having spoken to (now deceased) people directly familiar with the events at the time, they felt Flexner approached the non-allopathic schools with the intent of discrediting them.
Rockefeller philanthropy supplied key capital for the new model. The Rockefeller Institute for Medical Research (organized 1901) and the General Education Board directed tens of millions of dollars (enormous sums at the time) toward laboratory-based research, full-time faculty systems, and university-affiliated schools that met Flexner-style criteria. Frederick T. Gates, Rockefeller’s principal philanthropic adviser, viewed scientific medicine as a strategic social investment: it promised healthier, more productive workers and framed disease as a technical and biological problem rather than a social or environmental one. Rockefeller funding hence favored institutions that aligned with this biomedical approach; support for homeopathic or other sectarian emphases was withdrawn.
Note: E. Richard Brown’s critical Rockefeller Medicine Men (1979), provides the most detailed summary of what occurred here, but argues it was class-aligned philanthropy rather than a simple personal profit scheme and was framed by Gates as long-term institutional shaping, not a direct buyout of the AMA. That book and this article are the primary sources for the above section.
 Forgotten Home Apothec... Check Amazon for Pricing.
Forgotten Home Apothec... Check Amazon for Pricing. Finally, recently made available primary sources shed further light on exactly what happened. In 1911 Gates prepared five private “Notes on Homeopathy” reports exclusively for John D. Rockefeller Sr. These documents (now available through the Rockefeller Archive Center) harshly criticized homeopathy and its founder Samuel Hahnemann while praising William Osler and laboratory-based scientific medicine. Critics however noted that Gates overstated the reach of germ theory, misrepresented Hahnemann’s views on the body’s self-healing capacities, and asserted that homeopathy had never cured a single patient (despite hospital mortality data at the time indicating otherwise and Osler’s having publicly expressed respect for homeopathy). So, despite Rockefeller’s lifelong personal reliance on homeopathic physicians for decades and his repeated instructions that homeopathic institutions should receive “fair, courteous, and liberal treatment” equal to allopathic ones, the foundations under Gates’s influence (and later under John D. Rockefeller Jr.) provided no grants to any institution bearing the word “homeopathic” in its name. Abraham Flexner himself was later hired by the (Rockefeller) General Education Board to help implement the report’s recommendations, further concentrating societal resources behind the scientific model. Homeopathic schools, starved of capital and forced by licensing exams and equipment requirements to dilute their curricula, either closed or abandoned rigorous homeopathic training and by mid-century none remained.
Finally, recently made available primary sources shed further light on exactly what happened. In 1911 Gates prepared five private “Notes on Homeopathy” reports exclusively for John D. Rockefeller Sr. These documents (now available through the Rockefeller Archive Center) harshly criticized homeopathy and its founder Samuel Hahnemann while praising William Osler and laboratory-based scientific medicine. Critics however noted that Gates overstated the reach of germ theory, misrepresented Hahnemann’s views on the body’s self-healing capacities, and asserted that homeopathy had never cured a single patient (despite hospital mortality data at the time indicating otherwise and Osler’s having publicly expressed respect for homeopathy). So, despite Rockefeller’s lifelong personal reliance on homeopathic physicians for decades and his repeated instructions that homeopathic institutions should receive “fair, courteous, and liberal treatment” equal to allopathic ones, the foundations under Gates’s influence (and later under John D. Rockefeller Jr.) provided no grants to any institution bearing the word “homeopathic” in its name. Abraham Flexner himself was later hired by the (Rockefeller) General Education Board to help implement the report’s recommendations, further concentrating societal resources behind the scientific model. Homeopathic schools, starved of capital and forced by licensing exams and equipment requirements to dilute their curricula, either closed or abandoned rigorous homeopathic training and by mid-century none remained.
Note: I believe the reason the medical system (and scientific community) has been so strongly opposed to homeopathy is because it was the initial opponent the AMA had to vanquish to establish their monopoly—illustrating how often large actions create unintended consequences (as Rockefeller explicitly stated he did not want the status quo that followed).
In short, the combined effect of AMA organizational power, state licensing leverage, Flexner’s influence, foundation capital, and the deliberate withholding of support from competing systems monopolized medical education and practice by the science-focused allopathic model as alternative systems lost schools, licenses, and institutional legitimacy. Then, once the monopoly was established, the same institutions that had raised barriers to entry could define what counted as “real medicine,” what research received funding, and which therapies were branded quackery. Later federal drug regulation (e.g., the FDA) operated within this already-consolidated professional and educational framework.
When the above events are recounted, they are typically portrayed as the Rockefellers and the AMA attempting to monopolize medicine, both so that MDs could earn more (shifting them from being some of the lowest to highest paid members of society) and because Rockefeller had recognized that immense amounts of money could be made from the new scientific model of medicine (which is why he sought to enshrine it as the gold standard). I am inclined toward these arguments, both because Rockefeller and Carnegie had a history of brutal and methodical suppression of competitors when they established their respective monopolies in oil and steel (Rockefeller’s largely secret and conspiratorial, Carnegie’s more open) and because after their “philanthropy” medicine rapidly became a far more profitable enterprise. However, strictly on the basis of what the available sources substantiate, the outcome could instead be explained as a combination of unfortunate factors (most notably Rockefeller placing Frederick T. Gates in charge of his philanthropy), the broader institutional momentum that already favored laboratory-based scientific medicine and unscrupulous individuals quickly recognizing the immense profit potential of science-focused medicine.
Note: in the 1970s police raided and arrested Chinese immigrants practicing acupuncture (which was in high demand from the community).1,2,3,4 I vividly remember despondently asking someone who witnessed a raid “why are they doing this?” to which he said “the Rockefellers…control everything,” illustrating that this viewpoint has existed for a long time.
The AMA’s Monopolization of Medicine
Based on the events that happened, I believe it is fair to say the heads of the AMA quickly realized the immense financial value of restricting the practice of American medicine to allopathy. Furthermore, I believe they also recognized that it was in their financial interest to gain ownership (or at least a cut) of the therapies allopathic physicians could utilize at scale that could treat a wide variety of diseases, as beyond this being the most logical course of action for them to take if profit was the priority, numerous cases studies demonstrated it occurred.
Ultraviolet Blood Irradiation
Building upon the recognition prolonged sun bathing could cure severe infections (e.g., the 1918 influenza or tuberculosis) and that UV light was antimicrobial, in 1927, Emmett K. Knott discovered directly the blood to UV light cured a variety of otherwise fatal infections, and once he finally convinced doctors to try it, it was rapidly adopted across America’s hospitals because of how consistently it treated a myriad of challenging conditions including sepsis, pneumonia (including viral pneumonias), kidney disorders, asthma, polio, botulism, rheumatic fever, and viral hepatitis.
The pioneers of UVBI, in turn documented their work in a significant body of literature: 50 papers by 20 different authors (published in 18 different medical journals) covering over 3000 patients with 36 different diseases, all of which found remarkable UVBI benefits. In tandem, these results led to UVBI being promoted in mainstream media (e.g., The New York Times and Time Magazine).
The AMA then attempted to extort Knott by offering to conduct a study validating UVBI for $100,000 (approximately $1.4 million today) and to purchase the rights to Knott’s device in return for a small sales cut. After Knott refused (as did physicians across America advocating for UVBI—one of whom documented this in their records), the AMA decided to do the study anyway. It was overseen by a friend of the AMA director (who was designing a competing device) and curiously, prior to being done, JAMA announced it was likely to fail. The study had various issues (e.g., no one could inspect the machine, when returned they discovered a film had blocked UV light from reaching blood, it only had 68 test subjects, many cases were conditions UVBI wasn’t used for). Nonetheless, no adverse events occurred, no one died (despite many having dangerous conditions), and many patients experienced significant improvement.
Despite this, the 1952 study concluded:
“We have concluded that none of our patients derived benefit from the irradiation of blood with the Knott hemo-irradiator.”
Because of this “definitive study,” hospitals across America quickly abandoned UVBI and became fully committed to emerging antibiotic therapy. The large body of literature the pioneers produced was forgotten, Knott stopped producing his machine and then died in 1961.
Note: while the AMA successfully buried UVBI in the United States, it has been extensively used in Germany, Russia (and now China), with a large body of data showing it treats a wide of range of challenging and “incurable” conditions. One of the key reasons why I greatly dislike the AMA is because of how effective yet unknown UVBI is.
Krebiozen
Andrew Ivy, at the end of World War II, was arguably the most famous and influential doctor in America, to the point that the American Medical Association sent him as their representative to Nuremberg, where he helped draft the Nuremberg Code. In 1949 he was introduced to Krebiozen, a promising cancer therapy, and after seeing the evidence, became its leading proponent. Then, in 1951, while he was still testing it, a sensational press release went out claiming a major breakthrough, which immediately turned the medical community against him.
The AMA, recognizing its value, threatened the inventors to sell them the rights. When they refused, the AMA conducted a fabricated study to debunk it, hoping to bankrupt them and gain ownership. This was later corroberated by examining the actual records of the AMA study and by a co-conspirator plus another witness who testified under oath before the Illinois legislature about the criminal conspiracy AMA leaders had shared with him.
Ivy kept collecting data, including miraculous results for key politicians, and eventually showed in over 4,200 patients that Krebiozen had a 50-70% success rate depending on the metric used (but nonetheless, the AMA and then the National Cancer Institute continue to denounce Krebiozen).
When Ivy applied for approval, the FDA stonewalled them and eventually produced spectrographic data claiming Krebiozen was just a common worthless metabolite. Before long it was revealed the FDA had fabricated that data, leading to Senator Paul Douglas telling the Senate on December 6, 1963: “It is a terrible thing that we cannot really trust either the Food and Drug Administration or the National Cancer Institute.”
The FDA then used its new authority from the 1962 Kefauver-Harris Amendment to ban Krebiozen from being shipped across state lines on June 7, 1963, which led to large protests in front of the White House. They were on the verge of winning over Kennedy when he was assassinated on November 22, 1963, and Johnson could not be persuaded. Unable to get Krebiozen, many of those patients then died.
In 1973 Illinois outlawed it, and not long after, like so many other alternative cancer treatments of that era, it was forgotten. Fortunately, William Kronick, a well-known television producer, made an impartial program that documented this forgotten history and the FDA’s gross malfeasance throughout it.
Note: Mike Wallace of 60 Minutes also interviewed Dr. Ivy in 1957 (but I have not been able to find a copy of this TV program). Krebiozen was also featured in national magazines like Pageant, Argosy, and Inside Story.
The Koch Catalysts
Dr. William F. Koch was a chemist and physician who made a variety of discoveries (e.g., regarding the parathyroid gland) that were published in major journals. Eventually, suspecting cancer resulted from an abnormal (non-oxidative) respiratory cycle in cells and that natural catalysts existed in the body which could prevent this from occurring, he isolated those catalysts and observed remarkable recoveries in terminal cancer patients (and likewise, from the 1920s to 1940s other physicians corroborated these results).
Note: in addition to hearing many successful stories about Koch’s catalysts, I had direct experience utilizing two of them, and found they worked (and for conditions beyond just cancer)—making it quite frustrating this therapy was erased from history.
According to accounts from Koch and his supporters, AMA representatives approached Koch and attempted to acquire the rights to Glyoxylide which Koch refused as he wanted it to be easily available to humanity. In retaliation, Morris Fishbein, the powerful editor of the Journal of the American Medical Association, repeatedly denounced Koch as a quack in the pages of JAMA and used the full weight of the Association to destroy his reputation.
The FDA followed suit and pursued him aggressively, filing criminal misbranding charges (claiming his preparations were inert and worthless) and tying him up in lengthy court battles that spanned years. In two major trials (in 1943 and 1946) the defense presented numerous patient testimonies of dramatic recoveries (including many who’d been given months or weeks to live prior to the catalysts), with both ended without a conviction (a hung jury and a mistrial) with and leading to the cases being dismissed, and a few years later Koch moved to Brazil.
Note: In many accounts of the Rife technology (another therapy I’ve extensively utilized), it is claimed the AMA made a similar buyout offer to Rife, which he declined. After that, the AMA blacklisted the technology and the physicians using it. Rife’s company was hit with a costly lawsuit that effectively bankrupted it; the San Diego Medical Society warned doctors using the machines that they could lose their licenses, causing many to surrender the equipment; the FDA later investigated doctors using Rife technology and often confiscated their devices; and much of Rife’s work was lost when his laboratory burned down in a suspicious fire. While the AMA’s abrupt campaign against Rife after the technology had been gaining traction is well documented, no primary sources corroborate the alleged buyout attempt itself. This could mean the buyout story was added later to strengthen a suppression narrative, or simply that direct proof of that kind of covert blackmail is hard to come by.
Since it worked, the “doctored study” method used against UVBI and Krebiozen was applied to other therapies as well. In the 1970s the FDA aggressively campaigned against laetrile (amygdalin, claimed to selectively release cyanide in cancer cells), resulting in widespread confiscations and patients seeking it through back channels such as Mexican clinics. Amid intense public pressure to study it, Sloan-Kettering Institute assigned its renowned researcher Kanematsu Sugiura to test the substance. He conducted nine experiments across three spontaneous mouse-tumor systems and obtained consistently positive results, particularly inhibition of lung metastases. After NCI officials expressed doubt, further collaborative tests with other researchers (including a joint study with a skeptical researcher) were run; several of these also confirmed the metastasis reduction. Sugiura’s findings were nevertheless suppressed in the final 1978 published paper, which framed the overall outcome as negative, Sugiura’s positive results were attributed to a “unconscious bias,” and the NCI gagged on the topic thereafter. The cover-up was chronicled by Ralph W. Moss, the institute’s public affairs officer, who refused orders to falsify reports, organized an internal group (Second Opinion) to expose the discrepancies, and was fired.1,2
Note: The FDA’s primary soundbite for attacking laetrile was the risk of cyanide poisoning. While this toxicity was occasionally observed with oral use (due to gut bacteria releasing cyanide from the compound), it was never reported with intravenous or topical (DMSO) administration that bypassed the gut. Many practitioners over the years—including some with whom I currently correspond—have described these non-oral routes (topical with DMSO or IV) as remarkably effective against cancer, particularly when intravenous laetrile was combined with intravenous DMSO.
Lastly, the NCI’s use of this tactic against alternative cancer therapies was not unique to laetrile. With hydrazine sulfate, Dr. Joseph Gold had reported 40–50% positive results in properly conducted studies; the NCI’s own trials produced essentially zero benefit after patients were given substances Gold had repeatedly warned would cancel the effect. With Burzynski’s antineoplastons, the NCI diluted the compounds in its trials to the point of ineffectiveness while the FDA pursued an aggressive multi-year legal campaign against him. Finally, with Hoxsey, rather than running a controlled clinical trial, the NCI and FDA simply reviewed the case records he submitted, declared the documentation inadequate, and used those incomplete reviews to brand the therapy worthless (all of three of which, along with the other cancer stories were detailed here).
Likewise during COVID, to counter the wave of independent studies and clinical experience showing that inexpensive generic drugs like hydroxychloroquine (HCQ) and ivermectin could treat COVID-19, this playbook was run at scale, as doctored studies were published in the leading journals, then amplified in unison by the mainstream media, successfully convincing both the medical community and governing bodies these results were “the science.”
As a result, fabricated or systematically manipulated results were routinely published, the most notorious of which were the May 2020 Surgisphere-based papers in The Lancet and the New England Journal of Medicine that claimed HCQ dramatically increased mortality and arrhythmias on the basis of a massive multinational registry (successfully stopping HCQ trials around the world). However, their underlying data was so implausible the papers were retracted within weeks (after the authors could no longer vouch for the data), after which independent investigators determined the dataset had effectively been concocted out of thin air. Yet despite all of that, the episode still triggered worldwide HCQ trial pauses and policy shifts against HCQ.1,2,3,4
Likewise, the “Big Six” (later Big Seven) large ivermectin trials that hit JAMA, the NEJM and other high-impact outlets were riddled with design and conduct flaws engineered to guarantee failure: dosing too late, too low and far too short a duration, administration on an empty stomach, arbitrary weight-based dose caps that under-dosed high-risk patients, failure to exclude concurrent ivermectin use in control groups, mid-trial endpoint changes, long publication delays, and refusal to share individual patient data.
The Oxford’s PRINCIPLE trial went further, quietly reporting a statistically significant two-day faster recovery plus large reductions in hospitalization and Long COVID as a negative result by inventing a statistical threshold the same investigators had never applied to their own molnupiravir or budesonide arms.
Worst of all, in addition to fabricating data to show HCQ was toxic, patients were deliberately overdosed to provide that data. In the UK RECOVERY trial and the WHO SOLIDARITY trial, elderly hospitalized patients received HCQ at roughly 2,400 mg on day one followed by 800 mg daily. This was several times a standard therapeutic dose, above the threshold the UK’s own toxicology database flags as potentially lethal and resulted in markedly higher death rates (which were then used to prove HCQ was dangerous). Finally, a parallel Brazilian high-dose study had to be halted when nearly 39 % of patients in the extreme-dose arm died — and was nonetheless published in JAMA and in tandem with the Surgisphere trials. All of this, in turn, successfully convinced a large portion of the medical community one of the safer drugs in their arsenal many had routinely used for years was actually a deadly poison no one had noticed in the 65 years it had been on the market.
Note: all of this is discussed in much greater detail in Pierre Kory’s book The War on Ivermectin.
The FDA’s Monopolization of Medicine
In many of the previous campaigns, the FDA served as the enforcer once the AMA had successfully convinced the FDA or NCI (National Cancer Institute) that a therapy was “dangerous quackery.” However, after the passage of a 1962 law that gave the FDA broad powers to both approve and police medicine in the United States (which was done to prevent a subsequent thalidomide disaster), the FDA began enacting similar campaigns without an initial public instigation by the AMA (which for DMSO, I covered in detail here).
Note: this hence raises major questions as to who was behind this (e.g., was it always the Rockefellers or did the AMA heavily influence the FDA behind the scenes). While a consistent playbook can be seen throughout each of the cases I studied, the instigating party varied significantly (e.g., the AMA did not denounce DMSO until after the FDA went after it, and while DMSO eventually became a threat to the pharmaceutical industry, at the time the FDA did so, major pharmaceutical companies were heavily invested in bringing it to market).
When DMSO was discovered in 1961, due to how effective it was at treating a myriad of challenging conditions, it rapidly caught on, soon was being used throughout Oregon, and attracted major interest from both pharmaceutical companies (e.g., six of the world’s largest companies including Merck invested heavily in clinical trials) and the public as the media stories aired depicting it as a potential wonder drug.
Initially the FDA was very receptive to approving DMSO, but at a 1964 meeting (with the FDA scientist who stopped thalidomide), she both expressed that the FDA wanted to do everything possible to permit further testing of DMSO, but also that they were worried about being overwhelmed by a large number of DMSO drug applications (due to the immense demand for DMSO and its vast number of uses), so they wanted more animal data before continuing human trials (despite extensive animal and human safety data already being there). A year later, the trial data was there for tens of thousands of patients, drug applications were submitted by major companies to the FDA, a DMSO symposium was held and demand for DMSO continued to increase resulting in over 100,000 members of the public bypassing the trials and just using it for themselves.
As the FDA was deliberating over what to do, in September (immediately after receiving the applications), one subject in a trial who’d been taking many other medications had an anaphylactic reaction (which was never linked to DMSO and has never been seen since), after which the FDA began terminating INDs. Following this, in November, a few animal reports emerged that DMSO could alter the refractive index in certain animal species (something never observed in over 37,000 human test subjects or any member of the public using DMSO), at which point the FDA immediately outlawed all DMSO testing and sent out a telegram to all embassies stating to the world DMSO could make you blind, at which point the press parroted the line the FDA had saved us from a thalidomide like disaster.
Following this, the FDA began sending agents to investigate the pioneering DMSO researchers to acquire incriminating records (often in an illegal manner) and the FDA under its new leadership (the director wanted to brand himself as a “tough commissioner” who kept the medical community in line to help the public) shifted to a posture of aggressively policing the use of unapproved substances and blacklisting scientists who conducted research the FDA did not approve of.
While this approach initially worked, a large number of scientists rebelled and began holding symposiums attesting to DMSO’s efficacy in a large number of conditions, public pressure on the FDA never stopped, and countries around the world became disillusioned with the FDA’s persecution of DMSO and resumed using it themselves. In the midst of this, an October 1967 study was conducted where prisoners were exposed to DMSO doses 3-30 times higher than what anyone would ever use (achieved by covering their entire body in DMSO gel daily for 14 or 90 days) and subjected to an extensive battery of tests—all of which found DMSO was completely safe (including for the eyes). Finally, in 1978, facing Congressional pressure, the FDA eventually approved DMSO for one indication, interstitial cystitis and at 1980 hearings, promised they would not put roadblocks to future applications, and that unlike interstitial cystitis (which had “well controlled evidence”) there simply was not yet sufficient evidence to approve the other applications.
As you might guess, in the nearly fifty years that followed, the FDA never approved a single DMSO drug application.
However, in 1994, in response to growing public outrage over the FDA’s suppression of natural medicine (e.g., gunpoint raids to confiscate vitamins), Congress passed a law that removed the FDA’s jurisdiction over natural supplements, and because of this, DMSO gradually became accessible again (and then due to the traction the series I wrote on it achieved, has begun returning to the popularity it had reached in the 1980s prior to the FDA erasing the public’s memory of it).
Note: one of the most interesting facets of this saga was that a journalist who interviewed numerous successive FDA commissioners discovered most of them knew almost nothing about DMSO beyond the FDA’s soundbites (despite DMSO being the most controversial drug in America for well over a decade)—not unlike how Fauci’s private diary and Scott Atlas’s memoir showed he knew very little about the current science on COVID-19. Remarkably, two years after leaving office in 1969, President Johnson (who appointed the FDA commissioner who went to war with DMSO) reached out to Stanley Jacob (the pioneer of DMSO) for help as he’d realized he needed DMSO for his own health.
Lastly, the FDA has engaged in similar tactics against a variety of other therapies which threatened established medical franchises. For example, after a natural low-cost revolutionary sleep aid was discovered (which unlike most options not only worked but also restored health rather than destroying it—as most sleeping pills sedate the brain and suppress restorative sleep), despite a vast body of scientific literature demonstrating its value for a variety of challenging conditions, the FDA went to war with it. Branding it as a dangerous date rape drug (despite there never being an evidence this was an issue), the FDA eventually convinced the Congress to outlaw this natural substance in 2000 (excluding allowing one extremely expensively formulation to be sold at the FDA’s discretion for a small number of sleep disorders).
Note: the reason I have not extensively discussed many of these therapies is because I believe providing extensive evidence for easily accessible ones (which takes a lot of time and I am still far from completing the initial round of) is the most effective way I can “make things better.”
Oxidative Therapies
One of the simplest chemical reactions is oxidation—the loss of electrons. This process frequently involves oxygen (or another oxidizing agent) accepting those electrons, often releasing energy in the process (combustion is a classic example of rapid oxidation). Animal cells, in turn, generate most of their energy through controlled oxidation in the mitochondria. In contrast, many microorganisms lack the same protective systems and antioxidant defenses found in human cells, making them especially vulnerable to oxidizing agents and as a result, a wide range of effective disinfectants work by oxidation. Some (such as dilute hydrogen peroxide) are relatively non-toxic to humans, while others that employ stronger oxidants like chlorine (e.g., bleach) are more damaging to cells because they both oxidize and chlorinate organic molecules.
Because of this, a variety of oxidizing disinfectants have been studies for their ability to eliminate virtually every known pathogen, in a test tube, topically over infections, and in many cases, once put directly into the body. In the process of doing that, it was observed that not only were infections treated, but a variety of non-infectious diseases also improved.
Of the oxidizing therapies, the most well-studied one is ozone (three oxygen atoms bonded together) and due to the breadth of what its applications can address, has been extensively studied (outside of the United States) for its use in a variety of conditions. Because of this, like I did with DMSO, I have been working day in and day out to compile and summarize every published ozone study as very few people are aware of the vast body of literature supporting its use.
To put this in context, from the first ten thousand studies I’ve reviewed, infectious disease (bacterial, viral, fungal, and surgical, spanning virtually every organ system in the body) was by a wide margin the most commonly studied application (as appropriately administered ozone typically resolved them). However, beyond that, ozone was repeatedly studied (and frequently reported to help) in chronic wounds and non-healing ulcers, surgical and post-operative recovery, a wide range of dental conditions, pain and musculoskeletal conditions (e.g., osteoarthritis, disc herniation, and low back pain), gastrointestinal and liver disease, respiratory illness, and cardiovascular conditions—much of which I believe results from ozone’s ability to restore microcirculation. Finally, many other areas have repeatedly been reported to respond to ozone as well, such as diabetes, cancer, dermatology, neurology, obstetrics and infertility, urology, and eye disease (along with sporadic but favorable studies on conditions as varied as thyroid disorders and osteoporosis).
However, in almost all cases if you bring up the subject of ozone, most people (having no idea these uses exist), they will fall back to the soundbite “ozone is a toxic gas” or to quote the FDA’s Federal Regulations:
Ozone is a toxic gas with no known useful medical application in specific, adjunctive, or preventive therapy. In order for ozone to be effective as a germicide, it must be present in a concentration far greater than that which can be safely tolerated by man and animals.
Note: ozone’s toxicity results from it being irritating to the lung’s mucous membranes (which is why medical ozone is never administered via inhalation) and because ozone is used as a surrogate marker for air pollution due to the fact the same process which generates toxic smog also produces ozone (something that does not occur when medical ozone is generated). Lastly, with all oxidative therapies, a therapeutic dose exists, and in nearly all cases where someone responds negative to them, it was due to that dose being exceeded.
The War on Chlorine Dioxide
One of the more recent additions to the oxidative therapy family is chlorine dioxide (ClO₂), a highly potent disinfectant routinely used as a non-toxic alternative to chlorine across water treatment, food and beverage processing, and hospital sterilization across the world. The EPA registered it for food and water use in 1967 and by the 1980s was recommending it over chlorine, largely because as unlike chlorine, it doesn’t generate carcinogenic trihalomethane byproducts when it reacts with organic matter.
Since ClO₂ is typically generated from sodium chlorite NaClO₂, once it started being successfully used as a medical therapy, the FDA (along with the media and virtually every other health agency) adopted the it was “toxic bleach,” likely owing to the fact bleach (sodium hypochlorite) had a similar name and formula (NaClO)—despite the two acting completely differently. So, much in the same way DMSO research was globally halted because it would “make people blind” (despite improvements in vision consistently being observed after DMSO use), the fact people were being “poisoned with bleach” (despite no evidence demonstrating this) was used to do the same to CDS—creating the curious situation where oral CDS is branded toxic when taken medically but not when used to purify what you then eat and drink.
Note: I have encountered numerous people who had temporary issues from excessive CDS doses. For this reason, I advise individuals to drop or lower their dose when reactions occur (whereas others view this as a sign “beneficial detoxification” is occurring and advocate for continuing).
Positive experienced with CDS and Pierre Kory learning CDS had faced a similar pattern of suppression to ivermectin inspired him to write a book on the topic, which in addition to documenting many of the proven uses for CDS, provides one of the most well documented example of how the medical system colluded to suppress a therapy that threatened multiple franchises.
Note: this book is not on Amazon and can only be ordered here.
From the book, I learned CDS therapeutic research began after an accidental discovery in the mid-1970s, when an inventor searching for a non-corrosive sterilizer for his ultrasonic cleaning tanks noticed that a persistent irritation on his hands cleared after he’d handled a chlorine-dioxide-disinfected tank. He and his family became the guinea pigs, and he went on to show it worked for a wide range of topical and mucosal applications such as wound healing, acne, warts, moles, nail fungus, scalp itch and other skin irritations, dental and oral care (including tooth whitening), and animal infections such as bovine mastitis—work the FDA supported rather than obstructed (e.g., the inventor described the agency as “a bit of a help”). Over the following decades he and his companies, conducted more than 300 studies and published 42 papers, and he secured patents along the way—beginning with his foundational 1977–78 method patent (Germ Killing Composition and Method, #4,084,747), which made small-scale personal ClO₂ production possible, extending across the 30-plus patents he held on chlorine dioxide products, and culminating late in life in a method for injecting tumors directly with chlorine dioxide.
In parallel, an unnamed defense scientist Kory interviewed shared that he learned of CDS in (frequently classified) government projects where he used it to sterilize food and medical instruments for NASA, inactivate nerve gas (with NaClO₂) and then learned through a defector the Soviets viewed it as “the ultimate antidote to all bioweapons.”
Note: when Jim Humble’s book on MMS (CDS) came out, a friend asked me to review it, after which I told her “this would probably be very helpful if a bioweapon was ever released,” which I later realized meant that it threatened too many franchises.
Later, when working on a steel project in Nigeria, he was asked to help contain a cholera outbreak, and after consulting a firm renowned for designing municipal water systems, deployed a treatment system that used chlorine dioxide in its post-treatment. This quickly contained the cholera as intended—but then local doctors reported that the water was also curing the town’s malaria, which made no sense to him, since malaria is mosquito-borne rather than waterborne. So, he flew in a blood-disease colleague, who confirmed under the microscope that the drinking-water concentrations of chlorine dioxide cleared the parasite from the bloodstream within hours. Before long he was deluged with people traveling from around the region to collect as much of the water as they could, which they also reported cured a host of other conditions besides malaria. After the Nigerian health minister came to verify the findings, the scientist was flown to neighboring Ghana to meet its king—himself a physician trained at London’s premier school of tropical medicine—who, rather than embrace the discovery, ordered him to cease the work: malaria, the king argued, was keeping the population in check, and eliminating it before the region’s high birth rate could be addressed risked a future famine. His team and equipment were then expelled from the country.
Note: while that account (and others in his book) relies upon individual testimony given to Dr. Kory that cannot be independently verified, as I show here, numerous lines of evidence corroborate that the ruling class has actively pursued population control, and that in multiples cases this was done with vaccines.
Not giving up, he shared that he began mailing sodium chlorite samples to engineers and expeditioners around the world including Jim Humble, who in 1996, while leading a mining expedition through the jungles of Guyana, had two crew members fall gravely ill with suspected malaria. With no medicine on hand, days from help and nothing to lose, he gave them drops of the sodium chlorite he’d received and within hours both had recovered. Struck by this, Humble began experimenting on himself and other locals with malaria, saw the same result, and worked out that when sodium chlorite meets stomach acid it forms chlorine dioxide. He then discovered it also treated many other conditions (e.g., typhoid, dengue and HIV) and in 2006 published a book. However, once word of the malaria cure reached Guyana’s government, Humble was ordered out of the country within a day, after (by his account) as the nation’s main pharmaceutical supplier threatened to cut off drug donations to the capital’s hospital if the cure became public.
Note: when Africa was being overrun with Ebola in 2014, ozone advocates Robert Rowen MD and Howard Robins DPM, at the president’s invitation, went to Sierra Leone on a medical mission trip and publicly chronicled what occurred as the trip progressed. There, they trained well over a hundred doctors and staff (including at the government Ebola treatment center) on how to administer ozone, but despite the president’s support, were abruptly blocked by the health ministry from applying it officially to patients for “unknown reasons” (that they suspected resulted from pharmaceutical pressure as numerous novel ebola therapies were being tested at the time). As there was no approved treatment for Ebola (and the majority of cases were fatal), healthcare workers treating patients (who were not always bound by the same government restrictions) eagerly sought ozone and in the documented ebola cases where it was used, recipients fully recovered (along with ozone appearing to prevent ebola exposures from developing into disease).1,2,3
Later, Dr. Enno Freye and his team tested a sublingual chlorine dioxide formulation on 500 malaria patients in Cameroon, reporting complete reversal of symptoms within two days. While traveling to launch a follow-up trial in Senegal, according to Freye (in an interview with Pierre Kory), he was arrested at Rome’s airport after cocaine turned up in a package handed to him by the officials funding the study, and was imprisoned in Italy for three years.
Note: while I was able to find corroboration online for certain parts of Freye’s story,1,2 I was not able to find any verification he was imprisoned.
In Freye’s absence, the study was retracted as having “never actually been conducted,” he was stripped of his adjunct professorship, and regulators pressured the manufacturer into pulling the product.
Note: Freye attributed his prosecution to pharmaceutical interests protecting the malaria-vaccine franchise. His Cameroon work and Senegal trial, in turn, coincided with the final push behind RTS,S (Mosquirix), the GSK malaria vaccine developed over three decades1 at a cost exceeding $750 million1 and funded largely by GSK and the Gates Foundation, which poured more than $200 million1,2 into its late-stage development between 2001 and 2015 before the WHO recommended it for African children in 20211—despite a Phase 3 trial in which efficacy against clinical malaria waned to roughly 39% over four years1 (undetectable by year three in earlier pooled data1), and which flagged three safety signals its own investigators couldn’t dismiss: excess meningitis and cerebral malaria in vaccinated children, and a doubling of all-cause mortality in vaccinated girls.1,2
Other forgotten malaria trials highlighted in the War on Chlorine Dioxide include a 1982 report of malaria disappearing from a Nigerian town after a chlorine dioxide water unit was installed, and the field records of Jim Humble and the practitioners he trained, who between them claimed to have treated well over a hundred thousand cases. But the most striking was what happened with the Red Cross trial in Uganda.
In 2012, Klaas Proesmans, then CEO of the Water Reference Center (a research arm of the International Federation of Red Cross and Red Crescent Societies), oversaw a study in Iganga, Uganda, examining the effect that sodium chlorite–purified water had on malaria patients. Researchers identified 154 patients who tested positive for malaria by finger-prick microscopy, gave each cups of the treated water, and re-tested daily. Within 24 to 48 hours, all 154 were malaria-free, with no reported side effects. As word of its success spread, the Ugandan Red Cross and the IFRC issued statements denying any official involvement and insisting no trial had taken place—while simultaneously conceding it had, by claiming their staff had been “duped” into giving patients “poison.” Most importantly, unlike the other malariga accounts, which rest largely on witness testimony (which you can never be certain of), this one was filmed start to finish (the protocol called for one of Uganda’s top filmmakers to document the entire trial) and in the footage below, Proesmans, who later denied it, states on camera that the study produced “100% cured people... within 24 hours to 48 hours.”
Note: as you might guess, the above documentary was deleted from YouTube
COVID-19 and CDS
I have long observed that people who ascend into power tend to lack creativity, and so once a playbook has been established, it gets reused ad infinitum. As such, their predatory practices are typically first tested on a marginalized group that lacks broad public support, then once no meaningful protest follows, the conduct hardens into an acceptable standard and is replicated on the general population.
This, for example, is how I was able to predict what would happen during COVID-19—as a similar dynamic had already played out during Fauci’s AIDS crisis, where treatments that physicians around the country reported were saving patients’ lives were stonewalled, while a toxic and largely ineffective antiviral was pushed through (which was justified by the ever-mounting deaths of the untreated patients).
As such, it was no surprise that once researchers around the world discovered chlorine dioxide treated COVID, what we saw with malaria pattern repeated. In July 2020, Bolivia, then suffering one of the highest COVID mortality rates in South America, grew tired of waiting on the WHO for a solution and passed a law legalizing oral chlorine dioxide, which its military and universities produced and distributed under protocol. Within six months the country’s outcomes were among the best on the continent. Yet, the Ministry of Health, citing the WHO, PAHO, FDA, and EMA, subsequently issued a statement condemning the law and declaring the compound unsafe, and the actual program data were never properly published. The published evidence Kory assembles points the same way regardless—a retrospective study in which 90% of 1,163 relatives living with infected patients took CDS prophylactically and reported no symptoms, a chart review of more than 1,100 outpatients reporting a 99% recovery rate with only mild and transient side effects, an Ecuadorian physicians’ report of 97% symptom resolution within four days, and more than 14,000 PCR-confirmed cases treated across Latin America by over 3,000 COMUSAV doctors with no serious adverse events reported—all of which was observational rather than randomized, since the controlled trials, as we’ve seen, were blocked.
Likewise, everywhere it worked, the people behind it faced retaliation. In Peru, the Chief of the COVID Command in an entire region was fired in 2020 for treating patients with chlorine dioxide, and a health official openly laughed at the idea of even studying it. In Mexico, a surgeon who reported a 99.6% success rate across 3,000 patients had his hospital’s COVID unit shut down. Once COVID started, Mark Grenon and his sons, who had spent a decade distributing CDS, were pursued by the DOJ at the FDA’s request, extradited from Colombia, and sentenced to years in federal prison. Similarly, the studies that might have settled the question were simply not permitted: a University of Colorado trial was rejected because “the FDA prohibits such research,” a Bolivian army-led randomized, double-blind trial that had already cleared two bioethics committees was denied without explanation by the country’s drug regulator, and a multi-country study collapsed after regulators in eleven nations issued warnings and bans (e.g., for “toxic bleach”) that made patient recruitment impossible.
It also bears mentioning that when Trump broached using internal UV for COVID by referencing a device Cedars-Sinai had shown improved COVID by putting UV light in the lungs by stating:
Supposing we hit the body with a tremendous — whether it`s ultraviolet or just very powerful light..And then I said supposing you brought the light inside the body, which you can do either through the skin or in some other way, and I think you said you’re going to test that too. Sounds interesting.
TRUMP: Right. And then I see the disinfectant, where it knocks it out in a minute. One minute. And is there a way we can do something like that, by injection inside or almost a cleaning. Because you see it gets in the lungs and it does a tremendous number on the lungs. So it would be interesting to check that.
The media immediately repurposed their CDS soundbites to claim Trump told everyone to inject bleach—and despite the fact this was never stated, the claim repeats to this day (e.g., the Biden campaign used it during the 2024 election and online commentators recently used it to dismiss criticisms of Fauci).
Beyond the fact independent investigators (myself included) successfully used UVBI to treat COVID-19 and that Russia, in clinical trials, demonstrated UVBI treated COVID-19, there is one even more remarkable aspect of this episode.
The one internal use of CDS the FDA has permitted to advance to testing is a NP001, an IV sodium chlorite formulation that in two placebo-controlled Phase 2 trials, extended survival in ALS patients (by nearly two years in the non-progressor subgroup),1,2,3 and for which Neuvivo filed for FDA approval in 2024. On its face it seems astonishing that the agency would forbid oral chlorine dioxide as “poison” or “toxic bleach” while permitting the same compound to be dripped (injected) into the bloodstream at higher doses. But if you take a step back, it makes perfect sense: NP001 is a costly, patented pharmaceutical that patients cannot make or obtain themselves, and its narrow ALS indication threatens no existing franchise—whereas cheap oral CDS, taken at home for anything, threatens many drugs which have already “paid to play.”
Likewise, while UVBI has never received FDA approval despite many attempts and successful trials, (less safe) extracorporeal photopheresis (UVBI of the white blood cells with a photosensitizer) is a well established therapy for T-cell lymphoma that is also sometimes used for refractory psoriasis (and costs 5-50 times as much as UVBI). Similarly, while DMSO alone has still not been approved for any condition besides interstitial cystitis, many different proprietary pharmaceutical therapies containing DMSO have been approved for a wide range of specific conditions.
Note: In The War on Chlorine Dioxide, Kory also details CDS’s reported use across a range of other difficult conditions—from herpes, sinusitis, and stubborn fungal infections to non-healing diabetic wounds, Fournier’s gangrene, autism and several metastatic cancers that had failed conventional therapy along with the vast community of users that has been created by the tireless work of individuals whose lives were changed by the therapy (many of whom faced significant persecution for promoting it). Due to the reactivity many patients I work with have to stronger doses of any agent, my use of CDS has been restricted to temporary use for infections (where I’ve repeatedly seen it work) rather than longterm use at higher doses for systemic issues (as I use other therapies for those cases).
Conclusion
Throughout this publication, I have argued that science’s priorities are fundamentally misplaced, as while it is a wonderful tool for elucidating the truth, once its focus shifts from discerning the truth to supporting a prevailing interest (which is almost inevitable once scientific research becomes too costly to conduct and too much money rides on the outcome of a study), the data is worthless.
For example, we require large randomized controlled trials (which cost tens of millions of dollars) for drug approvals under the logic they can eliminate small biases or measurement errors, yet ignore the fact small observational trials any clinician can independently conduct have been found to find the same results for clinically meaningful results and that large RCTs have been shown to doctor results so that they support their sponsors (e.g., artificially inflating safety and efficacy). Likewise, the FDA has long justified the tight control they exert over the need to protect the public from “the next thalidomide,” yet, as we saw with the COVID vaccines, they ignored a tsunami of red flags that were so common over half of the American public could see them (which has caused a generational loss of trust in the public health authorities). Instead, as internal documents show, gagged their own scientists who pointed out the data showed those dangers so that they could continue to claim the COVID-19 vaccine was safe so that they could push outdated and unproven COVID boosters that were unlikely to work and in many cases not even needed (e.g., children had no risk of dying from COVID).
In short, we have a medical system where we pay vast amounts of money for research pharmaceutical companies use to create costly pharmaceuticals we not only directly pay for, but also pay for both the harm they cause and the social cost of millions of Americans who live with the debilitating illnesses medicine cannot address. As a result, the costs of medicine keep going up, and the massive monopoly forecast by Rockefeller’s critics has grown to the point many of our institutions are wholly dependent upon perpetuating it regardless of the human and financial cost doing so entails.
As we circle back to where this all began, I’ve long been struck by the fact many of the therapies I use and try to bring public attention were discovered in America roughly a century ago, as this was a time when technology had advanced to the point many remarkable medical innovations became possible, but the censorship apparatus had not yet matured to the point medical researchers had a real fear of retribution if they studied novel therapies which could disrupt existing disease franchises, and research had not yet been siloed into narrow biomolecular pathways which could produce profitable drugs for specific franchises.
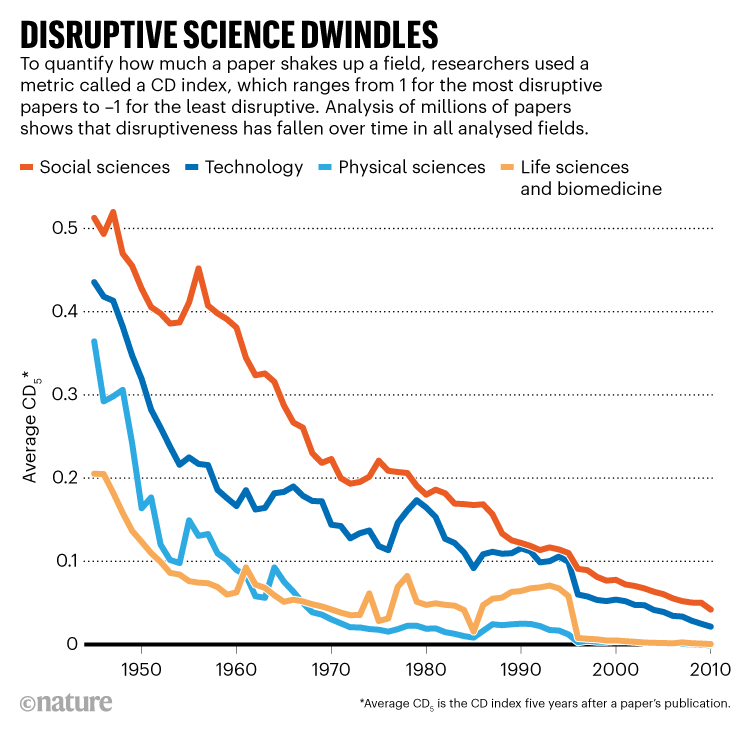
Somewhat analogously, many of the most remarkable and paradigm shifting discoveries in science were made by independent researchers who funded their own work and studied it outside of the scientific community. Now however, since so much money goes into scientific research and so many careers depend upon the status quo, novel paradigm shifting discoveries are quite rare, and as Nature recently highlighted, novel science which disrupts existing orthodoxies has rapidly dwindled.
It is for this reason that I think it is so important documented records like what Pierre Kory and Jenna McCarthy (who also writes on Substack) detailed in the War On Chlorine Dioxide are so important, as until we expose how again and again the medical cartel has used the same predatory playbook on us, it will continue to escalate far past what we saw during COVID-19. Imagine for a moment what the world would be like if our ever-evolving scientific apparatus was instead focused on discoveries which benefitted humanity and addressed our real needs rather than sustaining each disease franchise.
The therapies I regularly discuss here were discovered in America roughly a century ago with what is now fairly primitive technology. Yet, if that much was possible then, before we understood a fraction of what we now do, the real question is not whether medicine could produce miracles today. It’s why it doesn’t and why our scientific apparatus has shifted its focus from helping people to sustaining each disease franchise (which includes burying any potential competition).
It is for that reason that documented records like the one Pierre Kory and Jenna McCarthy (who also writes on Substack and helped make the book more accessible to a broader audience) assembled in The War on Chlorine Dioxide matter so much. Until we drag this playbook into the open — the way their book has — it will keep escalating far past what we saw during COVID-19.
Your support makes The Forgotten Side of Medicine possible! To receive new posts and support my work, consider becoming a free or paid subscriber.

