A recurring theme in human society is how frequently groups of people will hold viewpoints that are diametrically opposed to another group yet both groups will be absolutely certain they are completely correct and the other is completely wrong. In each instance, this means that at least half of the people involved are wrong and incapable of seeing evidence repeatedly presented to them which shows this.
For example, consider the recent drama that unfolded after ACIP's decision to reevaluate the newborn hepatitis B vaccine, where for context:
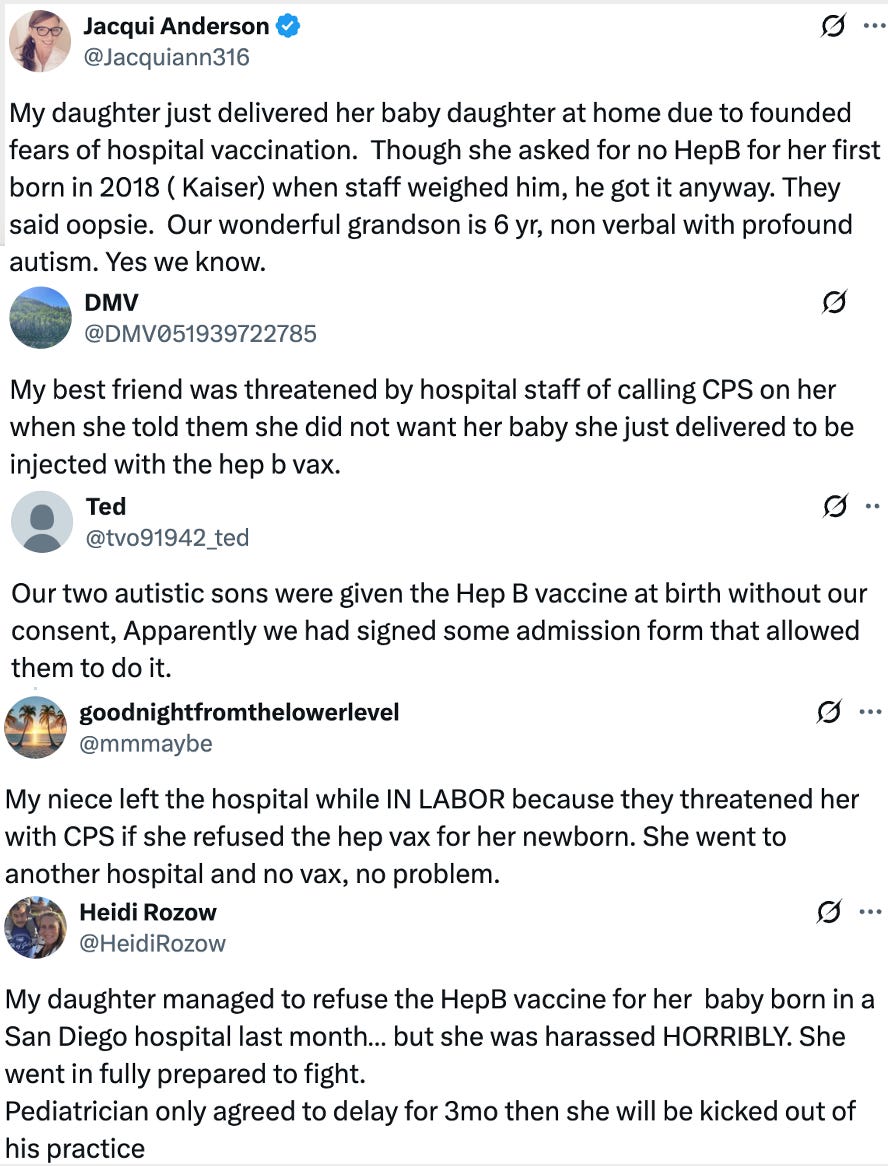
•Many people have believed for decades that significant harm results from newborn hepatitis B vaccine and that mothers who give birth at hospitals are routinely forced to vaccinate their children for it despite not wanting to.
•While significant observational data suggests this harm, as the FDA affirmed at the ACIP meeting, no controlled studies have ever assessed if the harm exists (despite their having been requested for decades).
•The public justification for newborn mass vaccination is that it serves as a safety net for the extraordinarily rare case (roughly one in a million) where a hepatitis B positive mother is not tested for hepatitis B, infects her child during childbirth, and the partial protection the vaccine provides is able to prevent the child from going on to develop a lifelong hepatitis B infection—despite there being no evidence thirty years of this policy has reduced hepatitis.
•ACIP’s new policy was to shift to making newborn vaccination optional for mothers who tested negative for hepatitis B.
While it seems like an open and shut case on what to do there, due to the way organized medicine behaves, I was doubtful this policy could be implemented, and for that reason, spent the last three months trying to help mobilize support for it.
Why is this? Quite simply, much of the medical profession is so invested in their way of seeing the world that they simply cannot see things which directly contradict it. Because of this, the (extremely rare) case of hepatitis B being contracted in unvaccinated children filled their entire mental focus, while conversely, the far more common (and frequently far more severe) injuries from the vaccines passed through one ear and out the other, and were all reflexively written off under the notion “no controlled studies demonstrate this, so that’s proof it’s not happening”—despite the fact controlled studies of vaccines are explicitly prohibited due to them being “unethical.”
As such, in the previous article I highlighted the ACIP meeting as I felt it illustrated an archetypal example of this psychological process and again and again, you could see every representative of the medical profession be completely unable to see anything but their own highly biased narrative on the safety and necessity of the hepatitis B vaccine.
Note: these are quite long, but throughout them, you can find examples of this close-minded behavior.
Likewise, once ACIP’s completely sane recommendation to stop vaccinating newborns of Hepatitis B negative mothers was enacted, it was treated as an existential catastrophe by both the medical profession and the media and a series of appallingly inaccurate expert interviews were aired to condemn this decision (e.g., Paul Offit, a former ACIP member, refused to attend the meeting to testify in favor of vaccines, then went on CNN and made a series of lies there, including claiming he was not invited to testify despite CDC records showing they made repeated attempts to contact him).
Of these, the most noteworthy one was that the ACIP chair, Hawaii Pediatric Cardiologist Kirk Milhoan MD, was fired from his position, as while he was highly regarded for his decades of service (and a severe regional shortage of his specialty where, in 2023, only an eighth of the needed doctors were present), the hospital instead chose to side with the deluge of complaints they received about the ACIP decision attempting to cancel Milhoan and fired him.
While much could be said about this, I wanted to highlight that:
•A key theme in Robert Mendelsohn’s 1979 Book Confessions of a Medical Heretic was that anyone who challenged the current dogmas of the medical field was expelled and treated identically to a heretic (e.g., consider how many doctors who tried to save COVID patients Fauci’s remdesivir protocols killed were then fired from their hospitals, had their medical licenses and board certifications targeted).
•It’s well recognized that doctors frequently only speak out against the medical profession or air unorthodox views at the very ends of their careers (to avoid being cancelled), and in this regard, the number of prominent mid-career doctors speaking out is extraordinary (e.g., for years the vaccine safety movement prayed we could have one well-recognized doctor advancing this message on a national stage; instead we have many).
•The largest victims of this cancel culture are patients as the doctors being excommunicated by the church of medicine are typically the ones they would most want to see at their most desperate moments when hospitalized (which is a key part of why the proportion of adults reporting a lot of trust for physicians and hospitals decreased from 71.5% in April 2020 to 40.1% in January 2024).
•As best as I can tell, his hospital no longer has an on-island pediatric cardiologist, which is particularly unfortunate now that more and more children are desperately needing this service due to the COVID vaccine myocarditis.
Note: when I posted this article, I assumed Milhoan was just fired from the Maui hospital (as I knew he was based there and since I didn’t have contacts there to ask, I just checked the island’s hospital director, saw he was not listed there and assumed that constituted proof he was fired). In reality, he had previously been forced to leave that position due to his COVID-19 related activity and this new firing was at a Texas hospital he sometimes worked at (presumably by periodically flying there). I apologize for the mistake.
Early Prognoses
Throughout my life, I’ve had the experience of being able to see what was in front of me, noticing that most people couldn’t regardless of how critical it was to observe. Eventually, after getting so fed up with men talking down to me when I raised these obvious observations (to make me submit to their worldview) I switched from being inclined to follow the crowd to being inclined to assume whatever the crowd followed was probably incorrect and prioritizing scrutinizing beliefs of that nature.
This confidence allowed me to begin seeking out others with a similar perceptual framework to my own (which I found constituted around 10% of the population) and to trust the implications of subtle patterns I was seeing. This for example was why when the COVID vaccines hit the market (and there was a near religious jubilation in my colleagues about them ending the pandemic and saving all of us) I cautioned those who asked to wait a bit before taking them as (based on Pfizer’s leaked regulatory data) I felt there was a high probability of long-term autoimmune and cancer issues from them.
Likewise, once they hit the general patient population, from the start, I noticed each day multiple patients came in reporting significant (but not fatal) complications they needed help with and had never experienced before from other vaccines and by the end of the week, I was certain enough the vaccines would be a huge issue that I notified a lot of (fairly hostile) people in my circle about it to encourage them to hold off vaccinating. Shortly after, friends around the country began contacting me to ask if the vaccine could cause sudden death (due to a friend or relative dying), and I made the decision to spend the next year verifying and documenting those injuries, as due to the fanaticism around the COVID vaccines, I felt it was unlikely anything would be published in any journal on it (which is essentially why this Substack went viral when I published it in February 2022).
Note: over that year, I saw numerous colleagues I highly respected continually dismiss every vaccine injury patients discuss with them—including cases of patients cancelling due to (in their relative’s word) them dying suddenly from the vaccine.
When I conducted that project, a few nearly identical cases jumped out to me, as it seemed as though the only possible explanation for them was mRNA vaccine shedding—something which by every known mechanism was impossible. For this reason, I made the decision in the original report I published to exclude all known shedding cases (along with two people I verified were magnetic who stated they had become magnetic after the vaccine) as while I suspected something was happening, I knew that would stretch the Overton window too far and cause the far more important point I was trying to convey (that the shots were injuring and killing people) to be dismissed as every critic of my central thesis would focus on those outliers.
As such, I spent the next year trying to collect as much evidence as possible shedding was occurring in a real and reproducible manner alongside looking at every possible mechanistic angle which could sensibly explain what was happening. Two years later, the Overton window had shifted enough for this to be an acceptable topic of discussion, and I spent a year working with Pierre Kory to bring attention to this phenomenon (as it is one of the strongest arguments against all mRNA gene therapies) and the case for it was strong enough that it’s now generally accepted within many circles we frequent.
This all touches upon a critical point—frequently to solve a problem, especially one the group assigned to it has failed to adequately address, you have to have the ability to see a wide sea of possible datapoints, and then have both the intuition and courage to know which ones to focus on and act upon.
Note: This trait characterizes many of the prominent COVID dissidents (e.g., two previously used this skillset to be immensely successful in the financial markets—and wealthy patients in those sectors have told me this skillset was the key to their circle’s success). This is why each of us immediately realized there was something very wrong with the vaccines, whereas most of our peers wanted the safety of the crowd and took much longer to be convinced a signal was indeed there. Put differently, our “filters” allowed us to see what was right in front of us—something which seems obvious in hindsight, but nonetheless the majority of the population was unable to do.
Why Reason?
Previously, I wrote an article describing my thought process on navigating controversial topics with a high degree of ambiguity. It specifically focused on how critical it is to avoid getting attached to any specific interpretation you have of what is occurring. This is both because, due to the ambiguity present, it is challenging to be sure of any interpretation (so becoming attached to a specific one becomes a barrier to seeing the truth) and because it is not healthy for your mind or spirit to covet and treasure some rare idea it has become in possession of.
However because this is not navigated, I routinely see people arrange a series of datapoints together into a logical chain which arrives at a predetermined outcome, despite many of those logical jumps not being rational (e.g., much more probable alternative conclusions can be arrived at from each data point). Sadly, once this happens, rather than simply be content with holding that belief, they frequently get very aggressive in pushing that belief onto others and slandering those who do not endorse it. Most importantly, this happens in every segment of human society (e.g., this is why I believe the CDC hid all their data the COVID vaccines were killing people), but remarkably, while most people can immediately recognize when others are doing it, they often lack the insight to see they are doing it.
All of this hence touches upon a major question. What is your actual basis for seeking to believe something? I would argue the most common reasons are:
•To eliminate discomfort from the world being difficult to understand (hence making plastering a simplified model onto it being preferable to a complex one which allows significant ambiguity).
•To seek out the comfort of belonging to a (belief holding) group.
•To validate one’s own ego and be “right about the world.”
•To gain power over others by having your truth dictate the flow of society.
Note: this ties into a view within evolutionary psychology that logical reasoning evolved primarily for gaining power within social groups rather than understanding the world and solving problems. Likewise, this highlights a frequent observation in psychology research—more intelligent (and successful people), while excellent at arguing their points, are reciprocally much less able to process (let alone act upon) data which contradicts their deeply held beliefs.
In my case, I had no interest in many of those (e.g., living in a world I fully understood makes life immensely boring and bereft of meaning) and in many cases (e.g., due to bad experiences with domineering individuals) I was emotionally primed against them. For these reasons (and getting quite frustrated with how often I had reached a conclusion I later learned was a product of faulty reasoning on my part), I decided the only path forward was to try to construct a functional means of discerning the truth of the world which was humble, flexible and well-designed enough I would gradually be moving towards the truth with.
Note: a major reason why I do not share many of the things I believe is because while I have enough certainty in them to be willing to act upon them, I think the potential I am incorrect is high enough I do not feel it is ethical on my part to share those views to a large audience, particularly since every year, beliefs I’d held for a long time shift as I learn more (plus, given the volume of content here it eats up a lot of time to correct errors I subsequently discover in past articles). Likewise, this is why I put a lot of focus onto the exact language I preface claims with (e.g., I suspect, I believe, or no qualifier etc.).
Information Overload
One of my colleagues has advanced a compelling theory to explain why a palpable madness seems to be gripping our society and more and more people seem to be going off the rails.
So much information is available now we are constantly bombarded with, that it has exceeded the processing capacity of the human mind. That is making a lot of people destabilize inside, and as the information glut increases, this problem will continue to worsen.
As mentioned above, I believe one of the basic safeguards the mind has to avoid this is by plastering a simplified explanation onto reality or siding with the crowd. Unfortunately, the current demand on the mind (due to the existing information load and the rate at which society now changes) is exceeding that buffer—so, as my colleague describes, we are beginning to see a lot of mental “glitches” emerge, many of us never previously encountered.
Fortunately, many meditation traditions have been aware of this underlying process over millennia and devised a series of methods to bridge that gap—many of which have been invaluable not only in my personal life, but also when practicing medicine and writing this newsletter.
Note: henceforth, I will use the term “subconsciousness.” Arguments can also be made that “unconsciousness” is more correct. I thought this over for a while, and I am ultimately not sure which should be used here.
Focusing on Value
In many environments you are in, a massive amount of data is present that the conscious mind cannot keep track of. However, to a large extent, the subconsciousness does and directs your focus to what in the environment has "value" for your conscious mind to be aware of.
One classic example is the "Cocktail party effect," where you can be in a room where many people are having conversations that blur together. Still, for some reason, you can immediately zero in on the one conversation where your name was mentioned. Most of you have probably experienced this numerous times, and the same principle holds in many other instances as well.
I have seen various explanations put forward to explain why the "Cocktail party effect" occurs, and from all of them, it's clear some part of the brain evolved to make this possible. One region that has been put forward as being responsible for this is the "reticular activating system." At this point, I don't know if the RAS is the region of the brain ultimately responsible for this effect, but going forward, I will state that it is to help convey the central points of this essay.
The filtering function of the RAS has been hypothesized to have evolved so that early humans could rapidly detect sources of food (e.g., berries) and danger (e.g., predators) in their environment. Since so much existed in their environment, and the stakes were high for missing many of them (e.g., a brief delay in spotting a predator could equate to death), the RAS was necessary. There needed to be an effective mechanism to rapidly draw attention to essential things while simultaneously not failing to observe any part of the environment.
Note: frequently when individuals have had strokes or some significant illness (e.g., car accident), part of their ensuing cognitive impairment (the ability to focus on things or recall information) results from the shock partially disabling the RAS, and if some type of protocol is done to restart it (e.g., stimulating the associated cranial nerve) this can often play a critical role in their recovery process.
We no longer have to deal with those high stakes in modern times, but the RAS persists. In turn, the "value" it seeks are often things our culture has habituated us to value, such as an opportunity for money, a product we want, or a potential mate (particularly since the widespread dopamine-focused marketing in our society revolves around conditioning the RAS to seek those things out).
In human interactions, recognizing the importance of the RAS is immensely valuable. This is because your words and actions are often far less important than what the other party has been primed to look for. Put differently, if someone's initial impression of you is positive (or they assess you as having value to them), their RAS will filter for things that show value in you. Conversely, if someone's initial impression of you is negative, their RAS will filter for signs you have no value and should be disregarded.
This is why people can repeatedly try to do everything right and make a positive impression on someone, but they are only seen negatively, and regardless of how hard they try, they keep looking worse and worse. Conversely, sometimes when you talk to individuals trapped in clearly abusive relationships (to the point outside observers can tell the abuse is happening), the abused party does not register most of the abuse and cites a couple of semi-decent things the abuser did as proof they are a good person, and sometimes will even try to defend the abuser once outside parties get involved. This might seem hard to believe, but like many of my colleagues, I've seen it numerous times in the ER (along with other areas of medicine).
Note: the concept I am describing here is often described as "confirmation bias" (where you only see things that conform to your pre-existing beliefs)
Filters Create Your Reality
One point Scott Adams helped bring general public recognition to is that we all hold filters (often arising from subconscious biases). Much of the reality we believe to be true is not representative of the objective reality. Instead, our notion of reality appears because our RAS makes us aware of things in our environment that affirm the reality we filter for. As a result, people come to believe their filtered world is reality because it’s what they see around them all day long. Scott Adams, in turn, refers to this phenomenon as two people watching the same film but seeing a completely different movie.
One of the things I hate about the media is how good it is at priming people to have a specific filter and then continually selectively feeding people only information that affirms that filter. I think my dislike of this comes not from the media’s behavior but the fact that so many people continuously fall prey to it, even when they are fully aware of it being done to them previously.
A few of the clearest recent examples of this media priming-and-reinforcement cycle are:
“The sky is falling because of COVID-19.”
“The COVID vaccines are 100 % safe, 95 % effective, and the only way back to normal.”
“Ivermectin is just horse dewormer and has no place in treating COVID—or cancer.”
“Trump is literally Hitler.”
“Biden is sharp as a tack and mentally fitter than ever.”
“Climate change means total societal collapse is imminent and already unstoppable.”
Although none of these were objectively true, because of how effectively the media primed much of the population’s RAS, many were left with a deep conviction that these filters were true and that the evidence for it was so overwhelming that anyone who could not “see” it was unforgivable. This, in turn, led to something I had not seen before with the American propaganda apparatus—families and long-term friendships were broken apart simply due to people having divergent viewpoints on these issues and not ascribing to the media’s narrative.
Note: One of the things I found the most surprising was just how effective this propaganda push was. The best example I can think of is how most medical professionals I met fell for all three. For instance, as James Miller (the honest doc I covered here) has highlighted in a national television interview after that article was published, many doctors and government leaders who directed the COVID-19 response established many of their beliefs on these narratives based on what CNN told them rather than reviewing the medical evidence themselves.
One of the things that gives me a great deal of joy in life is realizing that something I’d observed many, many times in my life had a quality I’d never recognized before, either because an existing filter removed it or because the complexity was beyond my present ability to grasp. This can hold for both very simple things (e.g., a blade of grass) and fairly complex ones.
For example, as the years went by, I began to gain a greater and greater appreciation for the fact most of human communication has nothing to do with the specific information being conveyed but rather is predominantly about what is going on in the body, mind, and spirit of each participant. Most of this is rarely overtly expressed but heavily influences both what each participant conveys and how they interpret what is said to them.
This is important because (unless you are very good with hypnosis) it is the realm where you have to focus to reach people who will not listen to what you say and the evidence you present. Furthermore, this broader spectrum of what’s contained within communication holds for every one of its mediums. For that reason, the primary thing I aim for here is to address those other areas of communication (e.g., I try to write in a heart-centered manner), as I feel all of that is ultimately much more important than the specific information of the subject at hand.
Note: all the above also encapsulates why online dating frequently leads to unsatisfactory outcomes for the participants. Conversely, one of the only upsides I’ve been able to identify to the COVID lockdowns is that they formed numerous stable-longterm relationships because newly matched couples were forced to spend that period directly connecting with each other rather than chasing all the (frequently dopamine-driven) distractions that pervade the society and prevent people from actually connecting with each other.
Another example can be seen in the practice of medicine. Since I was young, I loved puzzles, but as time passed, I realized all artificial systems have a predefined limit to the complexity they can reach. Conversely, with human beings, there is an almost unlimited degree of complexity present, and one of the key things that routinely brings me joy in practicing medicine is realizing something is present in the human system I had never recognized before despite having it staring me in the face with every preceding patient.
So, it’s for this reason that I often ask colleagues to send me (open-minded) complex patients they can’t figure out. For example, the COVID-19 vaccine disaster has been a remarkable educational experience as I’ve seen so many things go wrong in the body with these patients I never previously appreciated could go wrong in the first place. In turn, deeply looking into those problems opened my eyes to a variety of physiologic and subconscious mechanisms in the body I had never registered the importance of addressing before (and in some cases didn’t even realize existed in the first place).
Filters and Medicine
One of the subjects I’ve tried to bring attention to with this newsletter is medical gaslighting, the phenomenon where the medical system injures someone and then is told the injury is all in their head and had nothing to do with what the medical system did to them. On the surface, that sounds pretty bad, but unless you’ve directly experienced this, it’s hard even to begin to describe how awful it is to go through. Since this has happened to quite a few people close to me, I feel strongly about raising awareness on this issue.
From researching it, I’ve been able to establish that medical gaslighting has been a mainstay of Western medicine for at least 140 years (from the complications of mercury poisoning—which Western medicine used to give out like candy for everything), and I suspect but cannot prove it has a far longer history. Because of how long medical gaslighting has existed, I don’t think it is an issue specific to an individual doctor or the current medical industry’s monopolistic business model. Instead, I think it’s either a reflection of a malignant collective consciousness within the medical field or something intrinsic to human nature that becomes problematic once dangerous pharmaceuticals are involved. So I feel to end it, what is inside each of us is where the focus must lie.
The aspect of human nature most commonly cited to explain why doctors gaslight is that they understandably do not want to acknowledge medical injuries. This can either be for selfish reasons to avoid a lawsuit (although this is hugely misguided as patients are much more likely to sue when they feel they are being gaslighted) or because of how difficult it is for anyone to acknowledge they hurt someone else they wanted to help. This cognitive dissonance (the psychological defense mechanism that causes people to do this) is much greater for doctors as their entire identity (you have to give up a lot to become a doctor) is based around being bestowed with the ability to heal the sick, and society does everything to inflate that pedestal doctors are placed upon.
However, I do not believe cognitive dissonance is the primary issue. Instead, I would argue it’s an issue of filters. For example, a recent article on the overlap between the predatory behavior of the statin industry and the COVID-19 industry, I discussed how many unquestioned assumptions we all carry to navigate the world. As the complexity of your field increases, the number of assumptions you need to make increases as well. In medicine, it is virtually impossible to practice medicine without regularly utilizing a massive number of unquestioned assumptions.
For example, as I shared in there, despite the fact I’ve prioritized identifying erroneous assumptions throughout my career, I still frequently discover new ones I always assumed were true since I learned them in medical school. Because many of the assumptions taught during your medical training conveniently lead to concluding “pharmaceuticals (and other medical interventions) are not harmful” or “patients who believe they were injured by medicine are ill for a different reason,” it is inevitable gaslighting will occur.
Note: to illustrate, stomach acid is seen as a non-essential nuisance rather than being critical for digestion, which in turn is used to justify eliminating it with lifelong acid suppressing medications even though the easiest way to cure reflux is by increasing stomach acid so the stomach gets a signal to close its opening—something Senator Ron Johnson recently testified cured his reflux.
While the numerous unquestioned assumptions of medicine are certainly an issue, I believe they are a symptom of a much broader issue. It is immensely difficult to be fully aware of a complex system, so as a result, people typically “see” what their existing filters and all those unquestioned assumptions have been programmed to see.
When patients come in, typically, a lot is going on, and the most common response any physician will have during the brief visit is to cycle quickly through each filter they have been trained in for evaluating patients and see if any of those filters detect a disease the doctor knows to recognize. Since almost none of (pharmaceutically funded) medical training teaches you the filters for identifying pharmaceutical injuries (but it does teach the filters for recognizing signs of a psychiatric illness), doctors often can’t see the clear signs their patient has a pharmaceutical injury.
I have essentially found three ways to get around this issue, which I must acknowledge were adopted partially due to my personal history with medical gaslighting.
•Seek out and be trained in filters that identify complex medical conditions (e.g., mold toxicity or fluoroquinolone poisoning). This is doable, but there are a lot of filters to learn, and none of the standard educational pathways doctors go through expose them to the existence of these filters.
•View everything you see in the patient as a manifestation of some underlying process within their body and focus on identifying the underlying process rather than any specific symptom. This, in many ways, is the exact opposite of how we are trained to think in medical school, and particularly challenging because one particular underlying process can have a variety of different manifestations depending on the patient, which makes it very difficult to recognize what the unifying thread between all those symptoms is.
Note: here I discussed how I use a similar approach in my writing to explain complex issues as I try to boil things down to the core principles at work that everything else is emerging from.
•Have a perceptual framework that both provides the sensitivity to perceive the subtle signs a patient is providing to you and the ability to maintain an awareness of the entire patient rather than seeing them filtered diagnoses. In many cases, this is the only way you can perceive the critical diagnostic signs needed to assess the patient.
Perceiving Without Filters
Years ago, an acupuncturist told me that in ancient China (which had an enormous amount of warfare), there was a common saying—it is easier to raise an army of 10,000 men than to find a general to lead them.
Note: 10,000 was an idiom of the time that meant “a lot” rather than being a specific value.
I believe (although despite my best efforts, I cannot say with certainty) this quote gets at the fact that on a battlefield, there are so many different things occurring that if a general loses sight of one of them, that can be enough to crush their army and potentially decide the outcome of the war. For example, here are two lines from the Chinese classic The Art of War reflecting this idea:
To see victory only when it is within the ken* of the common herd is not the acme** of excellence.
Amid the turmoil and tumult of battle, there may be seeming disorder and yet no real disorder at all; amid confusion and chaos, your array may be without head or tail, yet it will be proof against defeat.
*ken means “knowledge, understanding, or range of sight or vision."
**acme means the point at which someone or something is best, perfect, or most successful.
Note: fictional works such as this also depict the view through which a general of that era saw the battlefield.
One of the significant differences between the modern era and many previous ones humans grew up in is that the world is much safer now, so there is much less pressure on individuals to have a continual awareness of their environment (e.g., leaders like CEOs often have very cushy jobs and far fewer people now have the basic survival skills necessary for if a war were to break out). As a result, much of this skillset has been lost, and people in turn, cannot apply it to the other areas of life it is often essential for.
“If you could be fully present to an ant for the time it took to walk down your nose, you would be enlightened.”
and
“If you could be fully present for the time it took a leaf to fall from a tree to the ground, you would be enlightened.”
are two common phrases in the meditation systems that reflect this same concept. Each of these phrases serves to illustrate the fact that there is so much going on around you at any given moment that your mind filters out that (while providing one with the illusion they perceive a continuous reality) that it is extraordinarily challenging to be fully aware of much of what is right in front of you.
Note: this issue is especially apparent in traumatized individuals who regularly disassociate.
In turn, innumerable practices were designed to gradually increase your awareness within each aspect of your being and each person and thing around you. These practices, in turn, all share many similarities since they reflect the same process.
This ability to be more aware of what’s around you comes more naturally to some. In medicine, those with this skill set tend to be the doctors who are most able to fully connect with the patient and recognize something they were never trained to look for. Conversely, this capacity greatly decreases as people become more disconnected from their bodies, deplete their nervous systems, and predominantly live in their minds (which sadly characterizes the modern digital age).
This, I believe, is one of the key factors explaining why older doctors who were not raised in the digital age tend to be better at connecting with their patients and seeing things their colleagues cannot recognize. Unfortunately, the entire push within medicine has been to have everything become automated (e.g., lots of tests and imaging or treatment algorithms doctors must follow) in place of the doctor creating a human connection with their patient and using that awareness to discern what their issue is.
I believe this transition has happened because it makes it much easier to sell billable medical services repeatedly. I also think it’s a shame it’s happened because a lot of conditions cannot be treated with the automated model, and I have lost count of how many people I and colleagues have seen who we felt had a relatively straightforward issue that dozens of respected physicians utilizing automated medicine were stumped on.
Note: one of the biggest factors I see changing this is AI, as much of what doctors have been automated into doing can be done by AI. As such, for doctors to retain their value to patients, they will need to go beyond algorithmically regurgitating guidelines (which AI is better able to do than human beings), and instead focus on the unique qualities only a conscious human can bring into a healing dynamic—particularly since COVID broke the longstanding unconditional trust doctors previously relied upon for patient compliance.
Filters and Information
When I was younger, I was a competitive debater, which often required arguing a point I believed was utterly incorrect. From doing this, I came to appreciate how it was possible to effectively argue almost anything if you correctly framed the debate and rearranged the available information to support your narrative.
This gave me a deep appreciation for how illusory "certainty" or "truth" was and how often things we were sure were true were simply the result of a selective presentation of reality. This is also why I've been so driven throughout my life to establish what is objectively true and not simply a subjective representation of reality…which is very challenging when you dive into it. Similarly, this is why when I write articles, before publication, I catch and address counterarguments that would be raised to them as my past training in debate made me able to take the role of someone who seriously disagrees with everything published here and is searching for ways to discredit the article.
I would now like to tie all the themes of this article together.
Whenever humans are exposed to an excessive amount of information (which can often be a surprisingly low threshold), they lose the ability to be present to all of it. Instead, their RAS uses a pre-existing filter that detects the parts of that information which have value to them.
In politics, this is often depicted through the concept of "nuanced ideas and simplistic truths." In the case of nuanced ideas, a few different premises need to be put together to understand the broader point the speaker is hinting at. In the case of simplistic truths, a single and simple premise (the audience most likely already agrees with) is instead stated.
The advantage of simplistic truths is that most audiences will understand them, and if they conform to the audience's pre-existing biases, they will emotionally support the speaker. The major disadvantage of simplistic truths is that they cannot address complex subjects. For many complex issues, were their nuance fully understood, most people on both sides of the political spectrum would likely reach a shared position they could agree upon. Instead, however, since only simplistic truths are utilized, things remain indefinitely polarized.
Sadly, when a nuanced idea is presented, many people can't put the individual premises together into a larger picture because they cannot be present to that much information at one time (or have emotional barriers to doing so). When this occurs, they often get angry, and search for an individual premise they can attack for challenging one of their simplistic truths.
Note: if you watch the evolution of American media over the decades, the time between transitions to new scenes has continually decreased which both causes and is reflective of a profound loss in the attention span of each American (and hence why I recently focused on the dangers of the disturbing trend within YouTube programming to use 1-3 second cutscenes on addictive children’s videos). Many of the qualities I’ve argued here are necessary to be able to perceive become much harder to perceive with a shortened attention span and part of why many members of modern society can’t follow nuanced ideas (and instead need simplistic truths to latch onto). Additionally, a good case exists that this loss of process capacity (e.g., ADHD often is a result of vaccine injuries), which in turn has caused the condition to become more and more common as the vaccination schedule proliferates throughout society.
Because of the need for nuance to address many of the polarizing and dividing subjects we face in this era, I decided to adopt that approach with this Substack. By virtue of being anonymous, I can do that here as it doesn't matter if people get angry at me, and even if they do, there is nothing for them to latch onto (this is also a big part of why I’ve never explicitly specified my gender as this society unfortunately causes many people to have negative projections to one gender or another—something I’ve personally experienced be directed towards me more times than I can count).
This greatly helps my mission because it makes audiences much more likely to try and appreciate the nuanced thought I present, rather than having the simplistic interpretation of "AMD is bad, therefore that idea is bad." Likewise, by going through the effort of understanding the idea (which I try to support as much as I can) it allows them to take personal ownership of it, at which point other people can take credit for it and allow it to diffuse throughout the society.
In most (but not all) cases, when someone's awareness expands to a broader reality than it is accustomed to within the body, mind, or spirit, there will be a natural strain created by it and a tendency to want to tense up and withdraw from that expansion. One of the best metaphors I have seen for this is the human response to pain, which people often cope with by tensing some part of themselves in response—even though the most effective way to mitigate pain is typically to relax into it.
Note: this is a foundational concept within Chinese medicine, as they believe blocked energy creates pain, and tension restricts the flow of the body's energy.
The process I am describing also regularly occurs with mental ideas. In turn, I would argue that this is what happens when someone has a response to a nuanced idea where they contract something inside themselves not to have to experience the strain of it being opened to a broader reality (e.g., by shutting their mind down and attacking the messenger). Although most commenters here are quite open to nuanced thoughts, I notice a common theme in their responses whenever I encounter a hostile party. They will not be able to see most of what I am saying, let alone appreciate the nuanced point being conveyed. Instead, they focus on a few statements within the response they can attack for violating their simplistic truths.
Note: I also think this describes one of the most common reasons why people become politically polarized as they do not want to make the mental effort or strain of being present of the other person (e.g., cognizant of their actual position) and instead want to take the mentally easy option of putting them into a box they can project their pre-existing ideas onto.
Because we live in an overwhelming sea of information, being fully present to all of it is nearly impossible. This forces everyone to utilize their own filters or filters provided by nefarious entities like Google. Since I have used the internet since its early days, I gradually acclimated to the ever-increasing flow of information and taught myself how to evade the increasingly sophisticated (and subtle) censorship—and to be honest, I am not sure what to suggest here for people who were not gradually habituated to our current reality.
The major challenge we all run into when we see a large pool of information is being present to it and knowing how to filter for its key points. Because there is no formal training or guidance for this, people typically focus on what their RAS is already primed to spot in a sea of information and whatever elicits a strong emotional trigger for them (hence why much of the internet is inane clickbait). Neither of these is very helpful if one's goal is to determine what is actually true. Instead, they frequently lead one to simply pick out (and often selectively interpret) the "facts" (which may be incorrect) from the broad sea of information that conform to their pre-existing biases.
The ways I have found to get around these issues are as follows:
•I have some type of intuition that tells me which thing (e.g., a data point, article, or book) I need to focus on in a broad set of data. Often I don't know why I felt pulled to it, but typically I discover very useful things from this process. Many people I've talked to who are successful analysts have told me they have a similar intuitive capacity.
Note: this is difficult to explain, but this process is not the same as having a bias to look for things that affirm your pre-existing viewpoints and it’s critical to not fall into that trap.
•I have gotten a natural sense of the biases behind different sources of information. I don't believe biases are intrinsically bad; we are human, so every source will have them (e.g., I am biased against the COVID-19 vaccines and upfront about it). However, it's important to consider what information a biased source puts forward due to its bias cannot be trusted and which can. This largely arose because I could “feel” the mind of many of the writers I read, and hence have an intuitive grasp of their bias.
For example, Wikipedia is a wonderful resource for non-controversial topics (e.g., summarizing medical or scientific concepts) no one would be particularly motivated to lie about. In contrast, on any commonly censored or controversial subject (including unorthodox perspectives on the previously mentioned scientific and medical concepts), Wikipedia's only value is learning the existing narrative. Similarly, I will often read a source I know is heavily biased against a subject I believe in so I can rapidly identify if there are any valid concerns presented by those skeptics (e.g., fact-checkers) I need to address or in some cases, cannot address and effectively disprove my belief (conversely if all the “arguments” they cite are ridiculous, I know I stand on strong ground with my point).
•It’s necessary to recognize when you have reached the point of diminishing returns with a source; if it is telling you things you already know, there is no value in reading it other than to confirm your existing beliefs. In a previous article, I mentioned that I spent a lot of time reading alternative literature (e.g., “conspiracy theories”). Still, I eventually stopped because I realized it was getting repetitive, and it reached the point where I would know most of an article's content shortly after I began to read it.
•Whenever possible, try to drill to the core of what the topic you are reading about actually is, and then search for the things that tell you what you need to know about that core as opposed to the countless superficial expressions of the subject (which can be almost endless to read through to). This is essentially the same process I use in many other facets of life, including working with patients (and when writing).
•Always consider if what is being presented can justify the claim. For example, a common way people who challenge the system are attacked is to make a variety of allegations against them which are based on assumptions, unproven allegations, inferences about the individual's state of mind, or hypothetical scenarios about the individual the author emotionally puts forward as fact, even though there is no way to know if any of that is true.
When all of these suggestive points are woven together, they can create a compelling narrative (especially if they are being read with a filter seeking to confirm a pre-existing belief). Still, when you cut through them, you often find nothing to substantiate them. Similarly, one of the things I realized over time with non-orthodox viewpoints (e.g., “conspiracies”) is that while many of them were provable beyond a shadow of a doubt, many others were a collection of speculative inferences and partial evidence woven together to argue for something you couldn't prove.
Many believe the two being blurred together under the same label ("conspiracy theories") was a deliberate tactic by industry (or the CIA). This was done so that whenever evidence was put forward showing industry did something very bad, rather than address it, industry could simply emotionally associate that evidence with the highly speculative conspiracies and thereby have the public emotionally dismiss the corporation's crimes.
Note: as mentioned above, writing here truthfully makes me very nervous because I am constantly worried something I put forward will either be incorrect or harm a significant number of people, and this has forced me to fact-check and question a lot of what I had previously thought I could just say (and had previously done so in numerous conversations).
•Allow your mind to expand so it can become fully conscious of a large amount of information without wanting to withdraw from it. I believe this skill is fundamentally the most important skill for navigating this entire issue.
At the same time, it is also the hardest to develop, and I owe much of my ability to do it to having trained the skill in areas unrelated to medicine or writing. However, if this is your goal, you can gradually move towards tolerating an increasing amount of ambiguity and excessive information without getting overloaded. Oddly enough, I have also found if you avoid substances, have healthy sleep cycles, use blue light filters on screens (e.g., f.lux) and stay away from unhealthy lighting (e.g., fluorescent tubes), your ability to be aware of larger volumes of information also increases.
Whenever I write here, I often have the idea of the article form in my mind, and what allows me to put it into text is if my mind can expand enough to be present to the entire piece. Frequently after this process begins, I will notice there are certain parts of the picture my mind does not want to look at and feel darker or as though they have shut down. This typically means that there is a contradiction or error in that part of my thesis I am trying to run away from and ignore. In turn, I find it is only once I get to the point I no longer feel that anywhere in my mental construct of the article that it is ready for publication. It took me a bit to realize this, but that process is very similar to what I had gone through previously with meditation practices, and that is likely where my approach to writing came from.
Note: one of the debates I always have with editors in writing is whether or not I should break up longer sentences. The argument for doing this is that it makes it easier to follow what I am saying. In contrast, the argument against doing so is that it breaks the continuity of the point I am making, and some of the meaning gets lost when the statement is fragmented. I am still not sure which is correct, but I currently default to the longer sentences.
To put all into context, right now I am in the middle of a project I really did not want to do, but felt had to be done ASAP so that MAHA could utilize it in time; manually reading and pre-sorting through tens of thousands of DMSO search results (I started this in late October after publishing the DMSO eye article on, I’ve done about 30,000 now and hope to finish before New Years). In turn, this has allowed me to find a lot of critical studies there was no other way to locate (e.g., a few days ago I found an obscure study which corroborated the remarkable results readers such as Daniel and numerous clinicians I’ve spoken to are getting for COPD and asthma).
Nonetheless, this has been immensely challenging to do (particularly given the time pressure on this), and has required me to use a lot of appropriately calibrated filters, maintain an awareness of everything I’ve gone through, and recognize when something inside me has impaired my capacity enough on doing this that I have to stop or switch to something else. I mention all of this because if I had not learned the strategies outlined in this article, there is no possible way I could have done this (and I felt I needed to explain to the readers here where my focus has been recently).
Conclusion
One of the most common political debates is if the Constitution is good or bad. The essential argument is that since the Constitution was written over 200 years ago, it is not suited for the modern world and needs to be replaced. The counterargument to this is that because the political system is so corrupt, anything that replaced the Constitution would be far, far worse than the current one (which has many positive things going for it).
Many spiritual leaders I have spoken to have shared a common concern with the modern era; that most existing religions are in the same situation as the Constitution. When they were developed, the world was very different (it was a simple agrarian society). The modern era has many unique needs and challenges, such as the insane overload of information and our over-identification with intellectual ideas. These changes are particularly concerning because they have replaced some of the most important things in life, such as our connections to ourselves (e.g., the digital age has made many lose the ability to feel) and those around us.
As a result, the current reality we face was never explicitly addressed within these texts. The world is so different now, no one could have predicted how things are at the time these were written.
For the same reasons, I do not support rewriting the Constitution, I also do not support revising the classic religious texts. However, there is also an alternative solution to this dilemma. Teach people to focus on grasping the timeless essence of those teachings by allowing their minds to expand enough to see the nuances within those texts rather than having a superficial reading that fixates on specific simplistic phrases and then rearranges them to support whatever the agenda is of the reader.
Our modern era is fraught with an immense number of challenges never seen before in history, and as such, it is necessary for us to navigate it with clarity and balance—particularly since things are so mutable now that our actions have become immensely impactful and able to easily ripple far into the future. I thank each of you for being on this journey with me and helping to assure we can work to shift things in a good direction.
----------------------------
Source
https://www.midwesterndoctor.com/p/seeing-truth-in-the-age-of-information



{kind=link}