UHC2030: The United Nations’ Global Public-Private Partnership For Healthcare

In the first part of this series, we looked at the United Nation’s (UN’s) Sustainable Development agenda. Contrary to most people’s perception of Sustainable Development Goals (SDGs), this agenda has little to do with environmentalism or reducing CO2 emissions.
Instead, it is a mechanism for introducing global governance and particularly global financial governance into every aspect of our lives and every corner of our society and polity. It enables the continuation of “the same debt imperialism long used by the Anglo-American Empire to entrap nations in a new, equally predatory system of global financial governance.”
Agenda 2030 was first outlined with General Assembly Resolution 70/1 (A/Res/70/1). In October 2015, this Resolution committed the UN to Transforming our world: the 2030 Agenda for Sustainable Development.
In UN parlance, “sustainability” is misleadingly used as a synonym for transformation. Nothing about the SDGs is as it first appears. The devil is omnipresent in the detail and, as with all SDGs, we should approach SDG 3, which the UN claims will “ensure healthy lives and promote well-being for all at all ages,” with considerable caution.
The UHC2030 Public-Private Partnership
The Universal Health Coverage agenda for 2030 (UHC2030) is a United Nations (UN) global public health initiative designed to achieve UN Agenda 2030 SDG 3.
UHC2030 claims to provide a “global platform and space for multiple stakeholders to connect, work together and influence national and international commitments.” The stated objective of these stakeholders is to make “quality health services available for all.”
In order to supposedly achieve SDG 3, UHC2030 brings together partners, or “stakeholders,” from both the public and the private sector to collaborate on the transformation of global healthcare. UHC2030 is a global public-private partnership (G3P) attempting to centralise worldwide control of healthcare.
In Part 1 of this series, we considered the 2016 report from UN-DESA, which found that G3Ps were not fit for purpose. The UN’s own investigators stated that a number of measures were required to make UN-G3Ps viable. Yet, to date, none of those improvements have been implemented.
UN-DESA noted that the commitment to G3Ps was “ideological.” The evidence shows that the UHC2030 global public-private partnership (UHC-G3P) is unlikely to deliver the claimed benefits. That is, if the real objective is to deliver quality health services to all.
Controlling public health policy and healthcare regulations at the world, national, regional and eventually local level is what the “sustainable development” of healthcare is all about. It is the “transformation” of healthcare everywhere.
So, who are the stakeholders and why do they want to “influence national and international commitments” to healthcare? Can they be trusted to deliver “quality health services” to everyone on Earth?
Or is there another agenda behind the stakeholders’ desire to transform our healthcare systems?
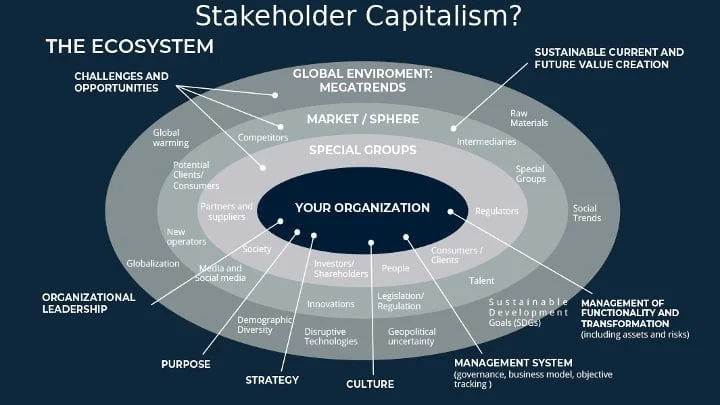
UHC2030 and Stakeholder Capitalism
G3Ps are formed of “stakeholders” based upon the idea, first promoted during the 1970s, of “stakeholder capitalism.” It proposes that the world will be a better place if multinational corporations act as “trustees of society.”
The legal definition of trustee: “the person appointed, or required by law, to execute a trust; one in whom an estate, interest, or power is vested, under an express or implied agreement to administer or exercise it for the benefit or to the use of another.”

Through the G3Ps that are set to provide “sustainable development” across the world, we are invited to accept that the Earth, all life and every aspect of our lives will be improved if global corporations are invested with the power to administer the entire global estate. The primary function of the governments we elect is to “enable” the transformation to take place.
The UHC-G3P consists of 83 national governments, including Iran, Lebanon, Somalia, Ghana, Uganda, Yemen, Myanmar, France, Germany, the UK, the US and Ukraine. Other nation-state partners contribute via multinational organisations.
For example, the Russian Federation is a UHC-G3P “partner” through the Inter-Parliamentary Union (IPU), International Labour Organisation (ILO) and the Asia-Europe Foundation (AEF). Similarly, China partners with the UHC-G3P through the AEF and Israel via the IPU. Numerous UN agencies, including the UNDP and the WHO, and various philanthropic foundations, such as the Bill and Melinda Gates Foundation and the Rockefeller Foundation, are also UHC-G3P stakeholder partners.
The primary UHC2030 objective is to “influence national and international commitments.” It is a G3P engaged in policy development. The subsequent “enabling environments,” funded by taxpayers, are enthusiastically endorsed by the UHC-G3P, which states:
National governments should progressively increase their investment in health by either moving towards allocating at least 15% of their annual budget to health, or up to 5% of their annual GDP[.] [. . .] This increased budget for health should be raised through mandatory and fair pooling mechanisms (such as improving tax revenue collection, setting up social health insurance)[.]
For most developed countries this won’t require any additional spending on their own healthcare. The majority already spend more than 5% of GDP. In 2020, the US spent nearly 19%. Germany was the second highest spender, devoting nearly 13% of German GDP to health.
The same is not true for developing nations. Many spend considerably less on healthcare as a percentage of GDP. Djibouti and the Democratic Republic of Congo spend just 2%, Pakistan and India around 3%. Sri-Lanka, Yemen, Syria, Egypt and Iraq are among the many other nations that would all need to increase relative healthcare spending to meet UHC-G3P sustainability targets.
UHC-G3P Debt for Healthcare Destruction Swaps
Low to middle income countries (LMIC’s) will need to either re-prioritise spending or significantly increase GDP, to create potential surplus, in order to meet UHC2030 demands. This is going to be difficult because these nations saw debt/GDP ratios escalate wildly as a result of the global policy response to the pseudopandemic.
The association between falling GDP and increased child mortality is well known. Prior to the pseudopandemic, many LMICs were already struggling to maintain precarious public health systems. The additional economic shocks had a predictable detrimental impact upon health care provision, especially for the most vulnerable.

The United Nations International Children’s Emergency Fund (UNICEF) were well aware of the risk. In July 2020, it estimated that an additional 6.7 million children under 5 would be pushed into malnutrition, suffering all the corresponding long-term health costs and higher associated mortality rates.
UNICEF noted that this disaster would be caused, not by COVID-19, but as a result of “the economic, food, and health systems disruptions.”
Yet UNICEF, a UHC-G3P stakeholder, inexplicably concluded:
The COVID-19 pandemic is expected to increase the risk of all forms of malnutrition. The wasting-focused estimates we present here are likely to be conservative. [. . .] The disruption of other health services during lockdowns will further compromise maternal and child health and mortality. [. . .] [T]he profound impact of the COVID-19 pandemic on early life nutrition could have intergenerational consequences for child growth and development and life-long impacts on education, chronic disease risks, and overall human capital formation[.]
There was no “profound impact from the COVID-19 pandemic.” None of the effects UNICEF described had anything to do with a respiratory disease. They were all the result of policy decisions taken in response to an alleged pandemic.
Knowing that the economic and health system disruption would kill vulnerable people, the UHC2030 multi-stakeholder partnership ploughed ahead with that disruption. They urged every government to invest more in COVID-19 response measures and treatments, as recommended by the WHO, a UHC-G3P stakeholder.
Bold emergency regulations and legislation were enforced. Inalienable rights were sacrificed and “collective responsibility” pursued. Patient safety—related to COVID-19—was prioritised by governments by providing financial support for “innovative solutions.”
The impact of this kind of “universal health coverage” on an LMICs, like Uganda, was devastating. With 74 alleged COVID-19 deaths per million of population (DPM), compared to a claimed 3,190 DPM in the US, Uganda didn’t have a pandemic.
Unfortunately, the shutdown of global supply chains and international markets by the developed nations, who claimed they did have a pandemic, hit Uganda’s economy hard. Ugandan export markets evaporated, businesses collapsed, unemployment soared as people were forced to migrate from urban areas to the countryside and return to subsistence farming.
As a lucky UHC2030 partner, the Ugandan government also had to borrow heavily to implement the supposedly necessary COVID-19 measures. It did so at the expense of preventative measures against other diseases like malaria, a disease that regularly leads to more than 260-280 DPM in Uganda.
Coerced into throwing everything at fighting a disease four times less dangerous than Malaria, Uganda also embraced additional public health risks. The Ugandan debt to GDP ratio in shot up from 22% to 41% in a single year and, by 2021, 9% of Ugandan revenue was spent on servicing its debts while GDP growth collapsed.
A report from The Center for Global Development revealed the effect of so-called “universal health coverage” in Uganda. It could be described as the evisceration of Ugandan healthcare:
Deterioration in essential health services[,] [. . .] reduced case finding for HIV/AIDS and malaria. Patients with chronic conditions who continuously relied on drugs for their survival [. . .] were unable to get their refills, while others could not afford medication due to lack of income. Patients who had been newly diagnosed with cancer were not able to be initiated into treatment. [. . . ] [A] majority of patients with these conditions faced an increased risk of complications and death due to inability to access healthcare[.] [. . .] These delayed initiations and interruption of treatment cycles resulted in increased stress, anxiety, disease progression, recurrence, and premature deaths.
In response to this man-made health disaster, as a UHC2030 stakeholder, the World Bank, decided that Uganda’s priority was to continue to invest in COVID-19 prevention measures it didn’t need. This kind of suicidal “economic planning” in response to a non-existent pandemic meant that LMICs like Uganda were crushed, not by COVID-19, but by the global policy response to COVID-19.
UHC-G3P Neocolonialism
The chances of many LMICs being able to meet the minimum 5% of GDP healthcare investment required by UHC2030 seems remote, unless they slash spending in other sectors. However, in partnership with the World Bank, the UHC-G3P suggest another way LMICs can meet its targets.
Debt restructuring mechanisms in Low-income countries and debt sustainability/reduction in Middle-Income countries.
In 2020, the G20 agreed a common framework for restructuring government debt. This built upon the previously established debt service suspension initiative (DSSI).
The DSSI enabled struggling LMICs to suspend bi-lateral sovereign debt repayment agreements in order to finance COVID-19 measures. The scheme ended in December 2021.
This made it possible for LMICs like Ghana to create the “fiscal space,” as described in Part 1 of this series, to enable UHC2030 sustainable healthcare. While population uptake of COVID-19 vaccines in Ghana has been low—at around 30%—compared to developed nations, by March 2022 AstraZeneca, whose major shareholders include Blackrock and Vanguard, had secured 57% of that vaccine market.
The AstraZeneca jab is not approved in most European countries due to the blood clots it has caused and irregularities in the limited trial data AstraZeneca released. Yet, unlike its mRNA counterparts, it doesn’t require hyper-cooling to store and transport and is therefore relatively cheap.
AstraZeneca and its fellow UHC-G3P partner, the UK government, made a loud public-relations noise about the claimed not-for-profit pricing of its COVID-19 jab. The Anglo-Swedish corporation signed the agreement on the provision that it could determine the date that it judged to be the end of the pseudopandemic. This factor, combined with its relatively inexpensive storage and transportation costs, made it the go-to jab for LMICs.
AstraZeneca struck a deal with another UHC2030 stakeholder, the GAVI alliance, and the Coalition for Epidemic Preparedness Innovations (CEPI) to provide, $1.3 billion of their vaccines to LMICs. These were supposedly supplied at cost, but it was a cost UHC2030 partner states like Ghana and Uganda could ill afford.
However, the DSSI temporary debt window enabled Uganda, for example, to pay considerably more for its 18 million doses of AstraZeneca jabs than the EU. It paid $7 per jab.
The production cost of the jab to AstraZeneca is unknown. Its development costs were met by UK taxpayers and their charitable donations. Its agreement to sell “at cost” to its UHC2030 stakeholder partner, the EU, saw it distribute the jabs at a unit price of $2.18.
The necessity for the more than 300% price hike for Uganda isn’t clear. It looks distinctly like AstraZeneca profiteered from the Ugandan, debt-based “enabling environment.”
UNICEF, a UHC-G3P partner, having warned about the disastrous health impacts of the economic decline caused by the cost of COVID-19 countermeasures, supported its UHC-G3P partners—AstraZeneca and the World Bank—by agreeing a deal, through the COVAX facility, for the supply of 170 million doses of AstraZeneca’s jab to LMIC’s.
AstraZeneca’s UHC-G3P stakeholder partner, GAVI, is focused on its state mission to create what it calls “healthy markets” for vaccines. GAVI notes that a “sustainable future supplier base is integral to the health of Gavi-supported vaccine markets.” Presumably, LMIC’s paying more than three times the market rate for drugs they don’t need is considered a “healthy market” by GAVI.
None of this predatory market activity, by its stakeholders, meets the UHC-G3P’s aim to:
Expand quality essential health services, strengthen health systems and mobilize resources in health in developing countries
For developing and middle income nations, the promise of “stakeholder capitalism” is an empty one.
UHC-G3P stakeholders appear to have manipulated LMICs, through their debt obligations, to invest in superfluous pharmaceuticals at extortionate prices. The multi-stakeholder partnership effectively weakened essential healthcare and increased population health risks.
From an LMIC’s perspective, UHC-G3P “stakeholder capitalism” looks more like corporate neocolonialism.
This is as expected because, as the UN knows full well, stakeholder capitalism doesn’t work as claimed. Public-private partnerships for public health are expensive, have a negative impact on healthcare and health outcomes, are prone to corruption and, broadly speaking, harm population health.
Why the UHC2030 global public-private partnership suggests otherwise requires explanation.
Improving Healthcare For Private Stakeholders
AstraZeneca are one among numerous pharmaceutical, healthcare and bio-technology corporations that are UHC2030 stakeholder partners. Other members include GlaxoSmithKline, Pfizer, Roche, Sanofi, Merck, Novartis, Novo Nordisk, Johnson & Johnson and Medtronic.
The stakeholder capitalism approach, rhetorically speaking, is exemplified by Merck who state:
As a global health care company that is committed to improving health and well-being around the world, SDG 3 is a core of our business and is aligned with our mission to save and improve lives. [. . .] We work in partnership with a range of stakeholders to improve the global health ecosystem.
Merck claims that it exists to save and improve lives by meeting SDGs. To do this it selflessly acts as a global health stakeholder. This is, perhaps, surprising because announcing a 28% sales revenue increase to $14.6 billion in its 2022 second quarter earnings report, Merck CEO, Robert. M. Davies, said:
Our strategy is working and our future is bright. I am very confident that we are well-positioned to achieve our near- and long-term goals, anchored by our commitment to deliver innovative medicines and vaccines to patients and value to all of our stakeholders, including shareholders.
So Merck isn’t entirely selfless. Making money is also important to the corporation, and especially to its shareholders who expect a profitable return on their investment. Consequently, Merck’s major shareholders, such as the global investment firms Blackrock and Vanguard, are also UHC-G3P stakeholder “partners.”
Pfizer, with its major shareholders including Blackrock and Vanguard, reported all-time high revenue, excellent profits and 92% operational growth in 2021, as a direct result of the pseudopandemic. Pfizer states how its commercial interests are well served by its stakeholder role within the UHC-G3P:
Pfizer believes in the promise of UHC. [. . .] As part of a series of bold moves, we have challenged ourselves to dramatically increase the number of patients that have access to our medicines by 2023. [. . .] We are committed to working closely with stakeholders and governments to accelerate these changes and improve overall access.
Through UHC-G3P, Pfizer is seeking to “dramatically increase” the size of its market. The “promise” of the UHC-G3P for Pfizer is that it can work with governments to “accelerate” its market acquisition programme.
The global investment firm Goldman Sachs is currently pushing investors to buy Pfizer stocks. The analysis that this advice is based upon does not reflect a belief that Pfizer will improve people’s health, but rather that people will stay sick for as long as possible and continue using Pfizer products.
In 2018, Goldman Sachs released its report titled The Genome Revolution. Looking to the potential for new genetic medicines to cure disease, Goldman Sachs were concerned that this would reduce long term revenue streams:
Curing existing patients also decreases the number of carriers able to transmit the virus to new patients, thus the incident pool also declines [. . .] Where an incident pool remains stable (eg, in cancer) the potential for a cure poses less risk to the sustainability of a franchise.
While Pfizer did great business during the pseudopandemic, the declining COVID-19 “incident pool” has seen its share price fall. Ongoing, long term treatment for chronic health conditions is what Goldman Sachs investors want from their pharmaceutical portfolios. Sustainability of the franchise, not improved public health, is important to these UHC2030 stakeholders.
This presents a potential problem to patients. While there is nothing wrong with making a profit, when those profits are based upon sickness, rather than health, evidently there is a conflict of commercial interest at the heart of the UHC-G3P.
As predicted by UN-DESA, UHC2030 has delivered “poorer quality services” that are “less accessible.” With multinational corporations acting as the key stakeholders, essential services are “less accountable.” We have already seen this in Uganda, Ghana and other LMICs.
Having degraded healthcare, the private sector won’t face any “penalty clauses.” The risk for their investors is “relatively benign” and will instead be shouldered by us—the taxpayers, both financially and in every other sense.
Consequently, it is reasonable to state that UHC2030 is a partnership for nothing more than global “health system governance” designed to enhance the centralisation of power over nation states for the benefit of the private sector.
The evidence suggests that the real purpose of UHC2030 is to maximise the number of sick people and keep them ill for as long as possible in order to maintain the “sustainability of the franchise.”
The UHC-G3P’s Impact Upon Developed Nations
Through UHC2030, the people in developing nations are set to endure continued neocolonialism. The populations in developed nations, especially the most vulnerable, can also expect similarly deleterious results.
Making a sustainable profit from healthcare is welcomed by UHC2030 stakeholding shareholders, such as Blackrock and Vanguard. However, private sector control of government policy and global health markets is an even more enticing prospect. For those at the top of the UHC-G3P’s hierarchical, compartmentalised structure, global health governance is a golden ticket.
The UN describe the September 2019 High-Level Meeting (UN HLM) on Universal Health Coverage (UHC) as “the most ambitious and comprehensive political declaration
on health in history.” One of the key commitments enshrined in the subsequent A/Res/74/2 was to ensure political leadership beyond health.
The UN-HLM declared that member states should:
Implement high-impact policies to protect people’s health and comprehensively address social, economic and environmental and other determinants of health by working across all sectors through a whole-of-government and health-in-all-policies approach[.] [. . .] Provide strategic leadership on UHC at the highest political level and promote greater policy coherence and coordinated actions through whole-of-government and health-in-all-policies approaches, and forge a coordinated and integrated whole-of-society and multisectoral response[.]
In addition to the reduction in healthcare quality, the UHC2030 global health governance policies are set to oppress the whole of society. This will be achieved by committing the whole-of-government to the “health-in-all-policies” (HiAP) approach.
In the US, the Center For Disease Control (CDC) explain how the whole of the US government has interpreted HiAP:
The places where people live, work, and play greatly impact their health. We can improve America’s health by working across government agencies and with private partners to create healthy and safe communities. [. . .] The Health In All Policies Resource Center supports a collaborative approach to health promotion that recognizes the importance of including health considerations when making decisions about things like transportation, education and other areas that impact our communities.
Private partners (multinational corporations, philanthropic foundations and NGOs) are empowered to work “across government” to define what they consider to be “healthy and safe communities.” These will be the communities that receive corporate services, purchase corporate products and advance corporate-funded NGO agendas.
Where, we live, work and play, the transport we use, our education and all other “areas,” in both our communities and our lives, will be engineered via the “decision making” of the UHC-G3P stakeholders.
In November 2021 the UHC-G3P leadership issued a statement in support of the WHO’s attempt to establish a Global Pandemic Preparedness Treaty. The Treaty is nominally a UK and EU led initative to establish global governance through “health security.”
The UHC2030 Steering Committee wrote:
Throughout the pandemic the linkages between universal health coverage (UHC) and health security have been clear. [. . .] Strengthening health systems, with a focus on primary health care, provides the foundations for both UHC and health security. [. . .] We are therefore pleased to share a new UHC2030 strategic narrative to guide advocacy and action on health systems for UHC and health security goals.
The associated report, titled “Action on health systems, for universal health coverage and health security,” is not available via the UHC2030 website but it can be found on the UK Government’s official site. The UHC2030 report is a “position paper” of the UK Foreign and Commonwealth Development Office (FCDO). The private sector is now fully embedded within the UK government.
The WHO definition of “health security” is referenced therein:
The activities required, both proactive and reactive, to minimize vulnerability to acute public health events that endanger the collective health of populations living across geographical regions and international boundaries.
The WHO lists a myriad of “public health events” that governments across the world need to prepare for.
These include, but are not limited to, rapid urbanization, environmental degradation, antimicrobial resistance, new diseases, chemical hazards, air pollution, poor nutrition, food-borne diseases, travel, economic interdependence, pandemics, other emergencies, weak health systems, economic shocks and, of course, climate change and population growth.
The whole of government shouldn’t simply react to such events but rather take measures to proactively “minimize vulnerability” to “public health events” that haven’t happened yet. As there is no aspect of society that doesn’t present the potential risk of a “public health event” occurring, perpetual population surveillance systems are required to keep us all “safe”:
UHC also involves [. . .] public health measures that prevent ill health [. . .] and provide health security. These include disease surveillance—including linkages to surveillance in the animal health and environment sectors.
Therefore, Global Health Security (GHS) is indivisible from Universal Health Care (UHC). The FCDO document continues:
Strong health systems form the foundation that underpins both UHC and GHS. UHC and GHS both need strong governance and leadership [. . .] adequate financing, the right medicines, and diagnostics, [. . .] strong community systems and good data and data systems for decision making.
Global health security is also best achieved through a global public-private partnership, according to the UK government:
Our programmes are driven by the science and conducted according to the best available evidence [. . .] drawing on UK and global expertise and public-private partnerships. [. . .] We will continue to work closely with important stakeholders such as professional and regulatory bodies, the research community (including research funders), the private sector, NGOs and civil society.
The ideological commitment to G3Ps clearly demonstrates that the health security agenda is not driven by the “best available evidence.” Something else is behind the push to install health security surveillance systems.
Speaking about “global governance for health,” the FCDO announced:
We will continue to play our part in getting the global health architecture in the right place to progress a more unified health systems strengthening [HSS] approach. [. . . ] We continue to use the important and influential fora, such as the G7 and the G20, [. . .] as we seek to tackle some of the most challenging global health issues. This includes shaping international discussions on global health security. [. . .] We will also actively seek to bring a HSS lens to conversations on wider international issues, which extend beyond the health sector, for example on climate change.
Everything—“wider international issues, which extend beyond the health sector”—can supposedly benefit from “global governance for health.” The UK government is among those that have already extended public health surveillance “beyond the health sector.”
In 2018, Public Health England claimed that climate change was “the greatest public health threat of our time.” The merging of climate change with public health was formalised in 2021 by then UK Health Secretary, Matt Hancock, when he announced the creation of the UK Health Security Agency (UKHSA).

UKHSA was created in response to the UK government’s alleged need to maintain a “relentless focus on our health security.” The government stated that it was “reforming health protection” to prevent and manage “health threats.” These reforms adopted the whole-of-government and HiAP approaches:
The reforms set out here aim to ensure that the public’s health is given the status it deserves – at the very heart of government’s priorities for action, policy and investment, nationally and locally, across government and across the NHS. [UKHSA] will work with academics and private organisations to ensure the latest behavioural science insights guide its work with citizens.
This placed the determinants of both national and local “policy and investment” under the centralised control of UKHSA. As a public-private partnership, this also gives UKHSA’s private sector partners influence over “policy and investment.”
UKHSA has taken over the function of Public Health England, NHS Test and Trace and the Joint Biosecurity Centre. Its surveillance systems are all pervasive. Practically everything is a potential public health threat:
The threats we face in future will be different; from new infectious diseases, new environmental threats or biohazards, to new behavioural challenges. So too will the opportunities to do more about them, through use of new technologies, analytics, cutting edge science and personalised behavioural approaches.
The people of the UK are the source of “behavioural challenges.” They will be deemed “biohazards” if they don’t follow UKHSA’s public orders.
UKHSA will work with its private sector partners to deploy “personalised behavioural approaches” to alter people’s behaviour if they don’t fall in line or refuse to comply. This is allegedly for the public good and will be delivered by the UKHSA public-private partnership:
We will be seeking to work in partnership with a range of public and private providers to develop and test cutting-edge incentivisation programmes that will help to support people in being healthy and active over the coming years.
UKHSA is the embodiment of the UHC-G3P “Health in All Polices” (HiAP) approach:
The factors most critical to good physical and mental health such as work, education and transport, housing and air quality [. . .] means that transforming public health requires very different ways of working across government. [. . .] Health will no longer only be the business of the DHSC [Department of Health and Social Care], but a core priority for the whole of government. [. . .] We will enable more joined-up, sustained action by national and local government and our partners.
Employment, travel, education, housing and even the air people breathe have all been transformed into “core public health priorities.” The whole of government will prioritise addressing the challenge of public health behaviour. Every aspect of life in the UK has now become the business of the UKHSA.
UKHSA claims that it possesses “world class health surveillance, joined-up data, horizon scanning and early warning systems” which enable it to detect new diseases and environmental hazards before they emerge. Consequently, UKHSA asserts the right to respond at “pace and scale” to “public health events” that don’t yet exist.
It also says it has the apparently magical ability to:
Mitigate infectious diseases and other hazards to health before they materialise, for example through vaccination and influencing behaviour.
Under the all seeing eye of UKHSA, the British will have to change their behaviour, economic activity and lives based upon UKHSA’s prediction of threats that will allegedly harm people if they don’t do as it commands. This SDG 3 based model is set to be repeated in every developed nation.
The whole-of-government, HiAP strategy is based upon the same circular reasoning common to all SDGs: we have to finance measures to mitigate fictitious events which might be bad if they ever happen.
Not only is this genuinely “Orwellian,” this form of extortion is also called a “protection racket.”
The UHC-G3P Command Structure
The private sector has primacy within G3Ps. Governments and intergovernmental organisations “enable” their business by directing public funds to create “fiscal space.”
The UHC-G3P is led by the “beneficial” owners of the private sector. We might look to Blackrock or Vanguard, for example, as representing the investors who stand to gain most from the SDG 3.
In turn, global investment firms are reliant upon the flow of capital and that is controlled by international financiers. This eventually boils down to the debt owed to commercial and central banks.
Ultimately, then, the UHC-G3P is controlled by the global banking industry. However, individuals need to be empowered to guide the SDG 3 project in the best interests of capital.
First and foremost the UHC-G3P is a global network. It is also a hierarchical, compartmentalised structure comprised of many different organisations.
Organised like a corporation, instead of a board of directors it has the UHC2030 Steering Committee. This sets the “overall strategic directions and oversight of UHC2030.”
Rather than a board of trustees the UHC-G3P has the Political Advisory Panel (PAP). The purpose of the PAP is to “strengthen political support for universal health coverage.”
PAP members achieve this by promoting the UHC-G3P agenda to “high-level political leaders” thereby “ensuring their commitment translates into action in countries.”
This leadership structure is “advised” by the UHC2030 Secretariat which is a partnership between the WHO, the World Bank and the OECD. Through the secretariat, UHC2030 has global power. The Secretariat terms of reference note:
Collaboration among the three agencies [WHO, World Bank, OECD] will leverage their respective mandates, convening power, unique organizational perspectives and strategic leadership to accelerate progress towards UHC.
Collectively, acting on the advice of the Secretariat, the Steering Committee and the PAP give direction to the UHC-G3P project. They have been empowered by the UN to hold centralised, global authority over the implementation of SDG 3.
The individual members of the Steering Committee and the PAP also have their own network connections to other organisations and groups. Through these affiliated individuals and high-level representatives, other private sector stakeholder organisations can also exert influence over the UHC-G3P and fulfilment of SDG 3.
The Managers of the UHC-G3P
Like any large organisation human beings are required to manage it. When we look at who has been given the responsibility for delivering SDG 3, extremely worrying questions arise.
Justin Koonin is both co-chair of the steering committee and a member of the PAP. He previously worked for the global accountancy giant PwC and is currently a “fund manager” for the South African multinational investment firm, Allan Gray. The company he serves specialises in asset investments in Africa. The UHC-G3P do not consider this an unacceptable conflict of financial interest in Mr Koonin’s case.
Alongside Rushinka Singhal, the Vice President of US-based Medtronic Labs, both a UHC2030 stakeholder and the world’s largest medical technology company, sits Edward Booty, CEO of Allied World Asia (AWA). Together, Mr Singhal and Mr Booty represent the private sector stakeholders on the UHC-G3P Steering Committee.
AWA is the Asian arm of Fairfax Holdings’ Allied World global insurance business. Allied World provide professional medical indemninty insurance to “health care consultants and companies that provide consulting services to health care facilities.”
The role of both of these “private sector” Steering Committee members is to encourage governments to finance enabling environments from which their respective corporations can profit. Again this is not considered a conflict of financial interest by the UN as it pursues its “business-friendly” policies.
Nor are ideological conflicts of interest an impediment to setting global health policy. Emilia Saiz Carrancedo is the founder of United Cities and Local Governments (UCLG) and a member of the PAP.
The UCLG she leads has embraced the communitarian civil society model. As a UHC-G3P stakeholder, UCLG provides another example of the intellectual dislocation required to believe any of the claims made about either SDG 3 or UHC2030.
On first reading the UCLG Global Agenda makes no sense at all:
UCLG believes that development and improvement of people’s living conditions should be undertaken primarily at the local level. We strive to achieve decentralization as a way to democratize public governance at all levels. [. . .] We aim to ensure that our values are shared among our members. [. . .] The major global development agendas can only be achieved if they are integrated into all planning, policy-making and action. [. . .] This is what we call localization: the achievement of the global agendas from the bottom-up.
According to the UCLG, led by Ms. Saiz, “localization” means total adherence to “global agendas.” Democracy is achieved through decentralisation as long as everyone agrees with UCLG’s globalist “values.”
The role of local communities, in fulfilling “global development agendas,” is limited to wholeheartedly agreeing with them. Beyond that, under UCLG’s global leadership, local communities have absolutely no say, nor any choice whatsoever.
UCLG is an exemplar of the civil society deception. If they weren’t so insidious and damaging to people’s lives, this kind of absurd organisation would be comical. The purpose is clearly to disempower local “communities” and disenfranchise the people.
The former Norwegian Prime Minister, Gro Harlem Brundtland, was among the founding members of the PAP. She is an avid eugenicist who firmly believes in elitist supremacy and population control, meaning population reduction.
Brundtland is a long-standing member of the influential globalist think-tanks the the Club of Madrid and the Trilateral Commission and is a founding member of the powerful think-tank, the Elders. She is both a former Director General of the WHO and a former UN Secretary General on Climate Change.
She rejects the scientific method and imagines that so-called “settled science” exists. In May 2007, Brundtland was asked about her thoughts on the climate debate. Commenting upon the climate reports offered by the UN and its intergovernmental climate body, the IPCC, She told gathered journalists:
This discussion is behind us. It’s over. The diagnosis is clear, the science is unequivocal — it’s completely immoral, even, to question now, on the basis of what we know, the reports that are out, to question the issue and to question whether we need to move forward at a much stronger pace as humankind to address the issues.
Brundtland believes that the foundational precepts of science—observation, inquiry and scepticism—are immoral. Like her fellow PAP stakeholder Emilia Saiz, she advocates a system of authoritarian, dogmatic control where people shut up and do as they are told by their superiors.
In 1987, Brundtland was the chair and lead author of one of the foundational documents for sustainability, Our Common Future. This report has been credited with coining the term “sustainable development.”
As a science-denier, it is likely that much of her contribution was ideological rather than logical. What became known as the Brundtland Report stated:
[S]ustainable development can only be pursued if population size and growth are in harmony with the changing productive potential of the ecosystem. [. . .] Painful choices have to be made. Thus, in the final analysis, sustainable development must rest on political will. [. . .] The ‘population problem’ must be dealt with in part by efforts to eliminate mass poverty, in order to assure more equitable access to resources. [. . .] Urgent steps are needed to limit extreme rates of population growth. [. . .] Excessive population growth diffuses the fruits of development. [. . .] A reduction of current growth rates is an imperative for sustainable development. The critical issues are the balance between population size and available resources [. . .] A nation proceeds towards the goals of sustainable development and lower fertility levels, the two are intimately linked and mutually reinforcing.
The commitment to population reduction is central to “sustainable development.” Everyone needs to grasp this. Sustainable development means reducing our number.
The “painful choices” will only be painful for some. The “political will” to reduce population will be exercised by those who define “the population problem” as they wish. There are many ways mass poverty could be “eliminated.”
The UHC-G3P for SDG 3 is effectively led by people who are ideologically wedded to the idea of reducing the global population and centralising their global authority over everyone.
So far, the pursuit of “universal health coverage” has seen a string of man-made public health crisis in developing nations and authoritarian mechanisms for social control rolled-out in developed economies.
This reflects the beliefs and objectives of the UHC-G3P leadership.
There is no reason to believe that UHC2030 can improve healthcare and no evidence to suggest that is even the intention.
Consequently “populations” should reject SDG 3 and those who seek to enforce it. The precautionary principle being the prime reason for doing so.
------------------------------
Iain Davis is an independent investigative journalist, author and blogger from the UK. His focus is upon widening readers awareness of evidence that the so-called mainstream media won't report. A frequent contributor to UK Column, Iain's work has been featured by the OffGuardian, the Corbett Report, Technocracy News, Lew-Rockwell and other independent news outlets. You can read more of his work on his blog: - https://iaindavis.com
---------------------------------
Source
https://unlimitedhangout.com/2022/09/investigative-series/uhc2030-the-united-nations-global-public-private-partnership-for-healthcare/



No comments:
Post a Comment