Did the Draconian Lockdowns Kill More People than Covid-19?
The lockdowns were foolish and illogical. Denmark closed its borders with Germany and Sweden when we had more coronavirus than they had. Golf was forbidden, which led to the absurdity that you were allowed to walk on the fairways if you didn’t look like a golfer. Tennis courts were closed, although gatherings of four people were not forbidden. Even outdoor running clubs closed.2 Life as we knew it stopped, on government orders.
There were early warnings but they were not heeded. After India introduced a lockdown three months into the pandemic, migrant labourers feared that hunger would kill them before the coronavirus did.3 Ten months into the pandemic, the World Bank estimated that it had caused an increase of about 100 million people living in extreme poverty,4 and poverty kills.
The pandemic saw a new breed of people who had become experts overnight but knew very little about the issues. They constantly appeared on TV with sinister messages about the need for lockdowns and many other interventions, including dressing whole populations as bank robbers with face masks, although they don’t work.5
Curiously, governments all over the world preferred to listen to the false gurus rather than to the real experts. I think it was because they supported the official narratives, ideas and dogma, which were flimsily created on the spot by politicians eager to be seen as powerful people who didn’t sit on their hands but did something.
The pseudo experts were also loved by the media. I wrote in a newspaper that after a year with the same Danish “expert” on TV, Allan Randrup Thomsen, a laboratory researcher, who was always worried and uttered trifles virtually every day about the pandemic anyone could have said, I needed a new remote control because I had used the mute button so much that it had stopped working.6 When I asked a TV journalist why they always interviewed Thomsen, he said it was because Thomsen was well prepared as he read what some journalists had written!
Only Sweden had a real expert the politicians listened to and respected, even after a public outrage7 when mortality figures became rather high in early 2020 compared with the other Nordic countries,8,9 which was because Sweden had failed to protect the elderly in the beginning. State epidemiologist Anders Tegnell stood his ground and advised that Sweden should not change its policy, which was to keep the society open and not mandate face masks, which were rarely seen in Sweden.
Sweden was a lone star in the darkness. I think it was the only country that didn’t panic and did the right things, and it had the lowest excess mortality in the whole western world during the pandemic9-11 (excess mortality is the increase in all-cause mortality during the pandemic compared with prepandemic levels).
The Panickers
The most harmful panickers were researchers from the Centre for Global Infectious Disease Analysis at the Imperial College London.12,13 The modelling exercises of Neil Ferguson and his team played a preeminent role in shutting down most of the world in early 2020, a couple of months into the pandemic. A year later, historian Phillip Magness wrote that the exaggerated forecasts of this modelling team “may well constitute one of the greatest scientific failures in modern human history.”13
I agree, and 2020 became the most surreal and shocking year in my whole professional life. The Danish Board of Health claimed it was documented that face masks were effective, which wasn’t true, and our government decided to kill all our 17 million mink only because a mutation had been found that might make future vaccines less effective, which was also wrong.2,14 In Denmark, we have four pigs for every citizen, and I asked in a newspaper: “What if our pigs got swine flu and there was a mutation in the flu virus? Should all our 25 million pigs then be killed? Where will this madness end?”14
Magness wrote that Ferguson’s team claimed credit for saving millions of lives through the lockdown policies and explained that they arrived at this figure through a ludicrously unscientific exercise where they purported to validate their model by using its own hypothetical projections as a counterfactual of what would happen without lockdowns.13
It became very dirty. Already one month after Ferguson’s model was published, researchers in Uppsala used it and showed clear signs of faltering. Later, at the one-year mark, Sweden had a little over 13,000 COVID-19 fatalities, smaller on a per-capita basis than many European lockdown states and a far cry from the 96,000 deaths predicted.13
In a House of Lords hearing, Ferguson snapped back, disavowing any connection to the Swedish results: “First of all, they did not use our model. They developed a model of their own.”13 This wasn’t true, but Ferguson continued deceiving people: “Imperial’s work is being conflated with that of an entirely separate group of researchers.”
Ferguson was dishonest. He had made country-level projections, which few people would find as they were hidden in an Excel appendix to the College’s report, and they showed that their results for Sweden were nearly identical to those of the Uppsala team.
How Effective Were the COVID Vaccines?
Yet again, the foremost deceptor was the team at the Imperial College London. They published a seriously misleading modelling study in a Lancet journal about the global impact of the first year of COVID-19 vaccination.15
It became the most-cited study of the number of lives saved, which they estimated as 14.4 million avoided COVID deaths and 19.8 million excess deaths, with remarkably narrow uncertainty intervals, which their data and methods did not allow: 13.7 to 15.9 million and 19.1 to 20.4 million, respectively.
In 2025, John Ioannidis and colleagues published a study that estimated that, during five years, from 2020 to 2024, the vaccines had averted 2.5 million deaths, with sensitivity analyses suggesting between 1.4 and 4.0 million.16
Considering that the College only looked at the first year of vaccination, the discrepancy between the two estimates is gigantic.
Even so, there were critical comments on John’s paper on the journal’s website that I agreed with and I also published my own.17 I noted that I had never seen a paper with so many assumptions before and that I found the estimates for vaccine effectiveness much too high, e.g. a reduction of 75% in mortality overall and 50% for the Omicron variant.
The essential issue is that there were, and always will be, too many assumptions for estimating the effect of the COVID vaccines on mortality reliably.
AstraZeneca’s Self-Congratulatory Estimates of Lives Saved
In March 2024, AstraZeneca withdrew its COVID adenovirus based vaccine from the market worldwide, officially due to a surplus of updated vaccines that targeted new variants of the virus,18 but with drug companies, we rarely know what the real reason is.
Many newspapers quoted an AstraZeneca statement that, “According to independent estimates, over 6.5 million lives were saved in the first year of use alone,” but strangely, not a single newspaper provided any link to the source.
As I got nowhere by searching on the Internet, I went to the company website where, mysteriously, I could not find anything either about the saved 6.5 million lives. But in a press release from May 2022, the vaccine, called Vaxzevria, was claimed to have “helped prevent 50 million COVID-19 cases, five million hospitalisations, and saved more than one million lives worldwide, based on model outcomes assessing COVID-19 worldwide.”19
These were monstrous lies. COVID-19 vaccines cannot prevent infection of other people because they produce IgG antibodies in the blood, not IgA antibodies in the respiratory mucosa.20 The whole idea of getting vaccinated to protect others, which we have heard constantly about in the media, is simply not true.
Interestingly, the 6.5 million lives saved were said to be an “independent” estimate, and the reference to the 1 million lives saved had only an internal reference: “Data on File Number: REF-131228.”
Non-traceable statements and unavailable data on file in a drug company should not be trusted and I could not find any of them, even though I searched intensely on the AstraZeneca website. But I found a press release from November 2021, six months earlier, which also claimed that 1 million lives had been saved.21 So, apparently no lives were saved between November 2021 and May 2022.
Pascal Soriot, AstraZeneca’s CEO, found it remarkable that a million lives were saved less than a year after the vaccine’s approval. So do I, but not for the same reason.
I suggest that Neil Ferguson and his team at the Imperial College London look for highly paid jobs in the drug industry. The industry also loves wild exaggerations about how dangerous diseases are and how many lives they can save. This is what they announce all the time. As I have explained, the drug industry doesn’t sell drugs, they sell lies about drugs.22
Can We See Anything on the Mortality Graphs?
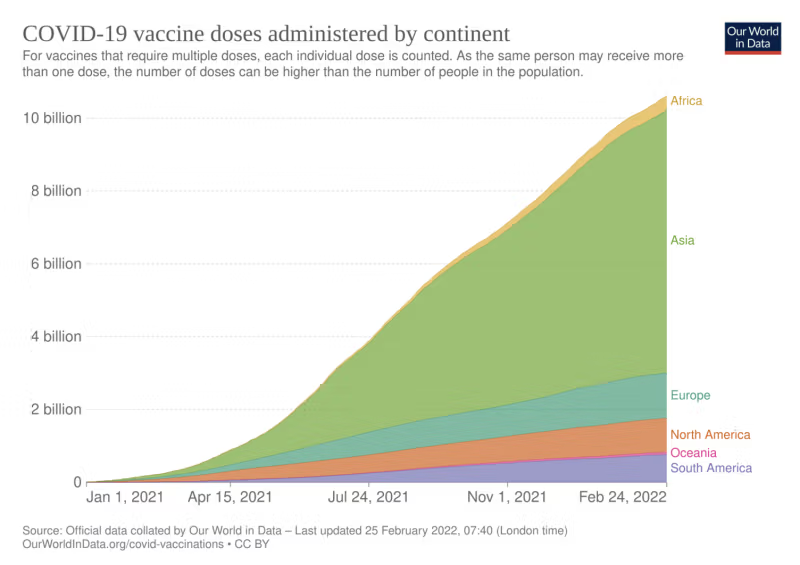
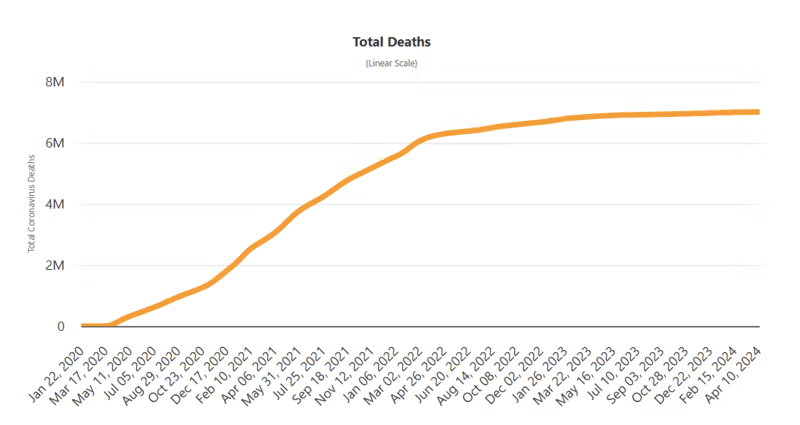
If the huge numbers of lives saved claimed by Ferguson and AstraZeneca were correct, it should be possible to see an effect of the vaccine rollout on mortality in a graph. But the cumulative vaccine rollout and mortality ascribed to COVID are both smooth graphs:23,24
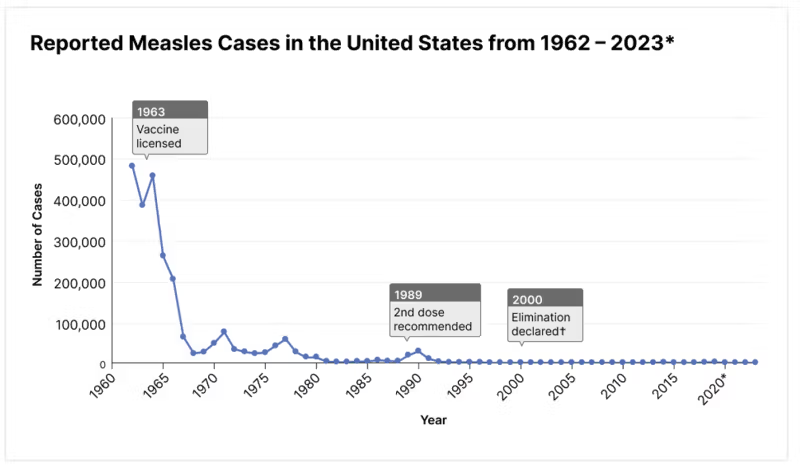
In contrast to the COVID vaccines, the measles vaccine is highly effective and when it was introduced in the USA in 1963, the incidence of measles dropped immediately and dramatically:25
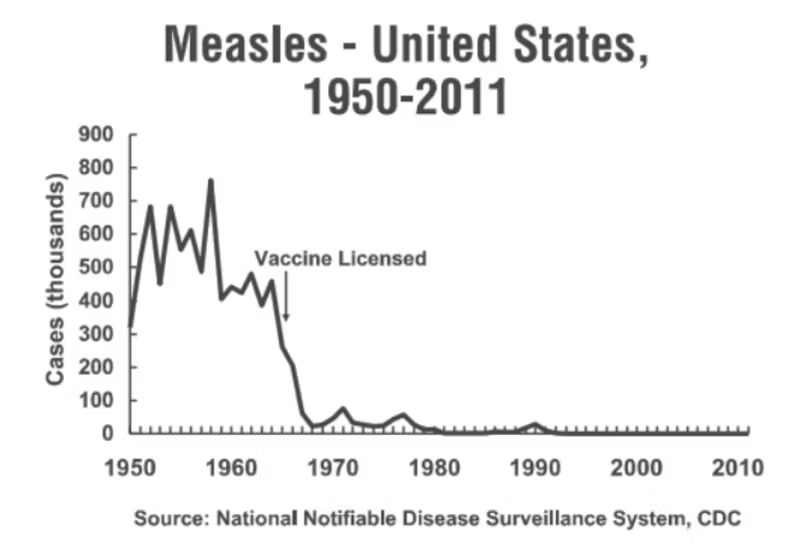
These data are from the CDC, which, in an earlier publication, showed a graph that went further back in time. It is no longer available but is included in my vaccine book.2 The graph shows that the measles incidence was rather stable before the vaccine came on the market (the arrow is misplaced, should be moved two years to the left):
The major differences to measles are that COVID-19 was caused by a new virus, highly likely manufactured in Wuhan,8,26 and that it was still spreading in a non-immune population when the vaccines were introduced, in December 2020 onwards. This makes it difficult to conclude anything about lives saved with the vaccines, but the graphs do not suggest any major effect on mortality.
People Killed by the Draconian Lockdowns
It is futile to try to estimate the number of lives saved by the Covid vaccines. There were far too few deaths in the randomised trials to be of any use and the uncertainties in observational studies are far too many and too large to allow trustworthy estimates.
But in the trials, there was an interesting difference between vaccine types. Overall mortality for the mRNA vaccines was not reduced, risk ratio 1.03 (95% confidence interval 0.63 to 1.71) whereas it was reduced for the adenovirus-vector vaccines, risk ratio 0.37 (0.19 to 0.70).27
One of the many uncertainties is that the virus mutates rapidly. Another obstacle is that the WHO advised already in April 2020 that:28 “A death due to COVID-19 is defined for surveillance purposes as a death resulting from a clinically compatible illness, in a probable or confirmed COVID-19 case, unless there is a clear alternative cause of death that cannot be related to COVID disease (e.g. trauma).”
This meant that some deaths ascribed to COVID were not caused by the virus, and the opposite was also true. Some people who died for various reasons without having been tested for COVID might have been killed by it.
The lockdowns killed a huge amount of people but we will never get anywhere near a realible estimate, for at least seven reasons.
First, as noted, lockdowns increased poverty dramatically.4 In an analysis by John Ioannidis and colleagues that compared 17 vulnerable countries defined as those with a low gross domestic product or large income inequality (which included the USA and the UK) with 17 other countries, there were 3,046 excess death per million inhabitants in the former group and only 500 per million in the latter.29
Second, it has been estimated, albeit in a modelling study, that lockdowns, lack of staff, and fear of getting infected increased maternal and child mortality in low- and middle-income countries so much that hundreds of thousands of lives have been lost.30 This is disastrous because it is loss of lives right from life’s beginning, childbirth, and the deaths of tens of thousands of young mothers. In contrast, the median age of those who died from COVID in the UK was 83 years.31
Third, people have died because they were not allowed to go to hospital, e.g. young people with meningitis.
Fourth, people have died because they were afraid of going to hospital, as they might get a COVID infection. Hospital avoidance behaviour has been documented for heart disease,32-34 which led to increased mortality for heart attacks35,36 and heart failure.34 In Hong Kong, emergency department visits dropped by 25% while the 28-day mortality of non-COVID-19 deaths increased by 8%.37
Fifth, the lockdowns increased risk factors for cardiovascular diseases, e.g. because of low physical activity, stress, and unhealthy diet, and for other diseases, too, e.g. psychiatric ones.
Sixth, living closely together increases the risk of dying from a respiratory virus substantially because people get a high infectious dose and therefore may not mount an adequate immune response before it is too late. This was shown for measles in ground-breaking research by Peter Aaby, both in Africa38 and in one hundred-year-old historic Danish data.39 During the pandemic, people were asked to work from home, and if infected, they were quarantined, which increased mortality. The index person – the one who gets infected in the community – will often have a good prognosis because of low viral load, but when that person is ordered to stay at home, secondarily infected people in the household will have a considerably higher risk of dying.
Seventh, deaths caused by the lockdowns are still occurring. For example, lack of cancer care may lead to shorter survival in future.
However, we could at least estimate how many lives that might have been saved, if other countries had had the same low excess mortality as Sweden. In the United States and in the United Kingdom, around 600,000 and 100,000 lives could have been avoided.40 These estimates agree reasonably well with the difference in population size. They do not take into account that many factors are different, e.g. many more people are obese in the US than in Sweden. On the other hand, that was also the case before the pandemic. Ioannidis estimated that the United States would have had 1.6 million fewer deaths if it had performed as Sweden.29
The Total Death Toll of COVID
Since we cannot separate virus deaths from deaths caused by lockdowns, we are left to estimate the total number of deaths the pandemic caused.
A study comprising the years 2020 and 2021 estimated that there were 6 million COVID deaths worldwide and 18 million (95% uncertainty interval 17 to 20 million) excess deaths (which include the COVID deaths).41 Another study, which also included only 2020 and 2021, provided a similar estimate, an excess mortality of 16 million (15 to 17 million).42
In Europe, 66% of the excess mortality during 2020 to 2023 occurred in the first two years.11 If we adjust the average worldwide estimate of 17 million for this, we get 26 million excess deaths.
The Economist has also estimated the total number of excess deaths in the world during the pandemic.40 A graph shows that the estimated number of COVID deaths was 7 million whereas the estimated number of excess deaths was 27 million, with an uncertainty interval from 19 to 37 million. This is remarkably similar to my adjusted estimate of 26 million.
The 34 countries studied by Ioannidis et al. had a total population of 983 million.29 If we extrapolate their 2 million excess deaths to the world, we get 17 million deaths. But as there were vastly more deaths in poor countries, this is likely a substantial underestimate.
Conclusions
The two current NIH directors have explained that we need a new pandemic playbook so that we don’t repeat the mistakes.43 The subtitle of their paper is telling: “The old one failed to cope with COVID and may even have caused it.” They outline how insane it was to allow the dangerous gain-of-function experiments in Wuhan with US financial support that rendered a harmless virus deadly.
The combined effect of fabricating the virus, the serious lack of appropriate safety precautions in the Wuhan lab in China, and the non-evidence-based draconian lockdowns created one of the worst man-made disasters ever in public health, with an estimated 27 million deaths.
China has killed many people before. The so-called Great Leap Forward under Chairman Mao is estimated to have led to between 15 and 55 million deaths in mainland China during 1959 to 1961. Mao’s so-called cultural revolution from 1966 to 1976 likely also caused millions of deaths.
For comparison, the number of deaths in the two world wars has been estimated as 40 million in WW1 and 70 to 85 million in WW2.
What I miss the most is for the WHO to call for a total ban on gain-of-function research. Perhaps there is a reason for WHO’s foot dragging.2 On December 31, 2019, Taiwan alerted WHO to the risk of human-to-human transmission of a new virus, but WHO did not pass on the concern to other countries. China had ensured that Taiwan is not a member of WHO, and WHO’s cozy relationship with China was criticised, particularly when WHO overly praised China’s handling of the coronavirus outbreak despite the fact that China did everything it could to cover it up.2,8,26
I consider this the biggest cover up in medical history and in the US, particularly Anthony Fauci also did what he could to deceive the public, which included lying to Congress and at a White House press briefing.26,44
The COVID saga demonstrates that the monomanic focus on just one disease increases deaths from other diseases. This is not public health and I wonder why the media have betrayed us to the extent they have, acting as uncritical microphone holders for our politicians without asking the relevant questions.
Time has come for the media to discuss the many millions of deaths all the unwise decisions have caused. We also need documentary films that can help us never forget what happened. Public memory is surprisingly short-lived.
References
1 Gøtzsche PC. Covid-19: Are we the victims of mass panic? BMJ 2020;Mar 8.
2 Gøtzsche PC. Vaccines: truth, lies, and controversy. New York: Skyhorse; 2021.
3 Kuloo M. “Hunger will kill us before coronavirus does”: Migrant labourers in Kashmir say
incomes have dried up and relief shelters are inadequate. Firstpost 2020;Apr 8.
4 COVID-19 to add as many as 150 million extreme poor by 2021. World Bank 2020;Oct 7.
5 Gøtzsche PC. False propaganda about face masks and Cochrane editorial misconduct. Institute for Scientific Freedom 2023;Sept 11.
6 Gøtzsche PC. Åbn Danmark igen, og gør det frivilligt at bære mundbind. Jyllands-Posten 2021;Feb 18.
7 Vogel G. Sweden’s gamble: The country’s pandemic policies came at a high price – and created painful rifts in its scientific community. Science 2020;Oct 6.
8 Gøtzsche PC. The Chinese virus: Killed millions and scientific freedom. Copenhagen: Institute for Scientific Freedom; 2022 (freely available).
9 Burström B, Hemström Ö, Doheny M, et al. The aftermath of COVID-19: Mortality impact of the pandemic on older persons in Sweden and other Nordic countries, 2020-2023. Scand J Public Health 2025;53:456-64.
10 Gøtzsche PC. Sweden did exceptionally well during the COVID-19 pandemic with its open society. Brownstone Journal 2023;March 28.
11 Pizzato M, Gerli AG, La Vecchia C, et al. Impact of COVID-19 on total excess mortality and geographic disparities in Europe, 2020-2023: a spatio-temporal analysis. Lancet Reg Health Eur 2024;44:100996.
12 Ferguson NM, Laydon D, Nedjati-Gilani G, et al. Impact of non-pharmaceutical interventions (NPIs) to reduce COVID-19 mortality and healthcare demand. London: Imperial College, UK Govt 2020;March 16.
13 Magness P. The failure of Imperial College modeling is far worse than we knew. The Daily Economy 2021;April 22.
14 Gøtzsche PC. Har mundbind nogen effekt? Og hvad med minkene? Eller svinene? Dagens Medicin 2020;Nov 9.
15 Watson OJ, Barnsley G, Toor J, et al. Global impact of the first year of COVID-19 vaccination: a mathematical modelling study. Lancet Infect Dis 2022;22:1293-1302.
16 Ioannidis JPA, Pezzullo AM, Cristiano A, et al. Global estimates of lives and life-years saved by COVID-19 vaccination during 2020-2024. JAMA Health Forum 2025;6:e252223.
17 Gøtzsche PC. Too many assumptions for estimating the effect of Covid-19 vaccines on mortality. JAMA Health Forum 2025;Sept 12.
18 Davey M. AstraZeneca withdraws Covid-19 vaccine worldwide, citing surplus of newer vaccines. The Guardian 2024;May 8.
19 Vaxzevria approved in the EU as third dose booster against COVID-19. AstraZeneca Press Release 2022;May 23.
20 Siri A. Vaccines, Amen. The Religion of Vaccines. Injecting Freedom LLC; 2025.
21 Two billion doses of AstraZeneca’s COVID-19 vaccine supplied to countries across the world less than 12 months after first approval. AstraZeneca Press Release 2021;Nov 16.
22 Gøtzsche PC. Deadly medicines and organised crime: How big pharma has corrupted health care. London: Radcliffe Publishing; 2013.
23 COVID-19 vaccine. Wikipedia 2024;June 18. Data from Our World in Data.
24 https://www.worldometers.info/coronavirus/.
25 Measles cases and outbreaks. CDC 2025;Nov 19.
26 Gøtzsche PC. Origin of COVID-19: The biggest cover up in medical history. Brownstone Institute 2023; Oct 9.
27 Benn CS, Schaltz-Buchholzer F, Nielsen S, et al. Randomized clinical trials of COVID-19 vaccines: Do adenovirus-vector vaccines have beneficial non-specific effects? iScience 2023;26:106733.
28 International guidelines for certification and classification (coding) of covid-19 as cause of death. WHO 2020;April 20.
29 Ioannidis JPA, Zonta F, Levitt M. Variability in excess deaths across countries with different vulnerability during 2020-2023. Proc Natl Acad Sci USA 2023;120:e2309557120.
30 Roberton T, Carter ED, Chou VB, et al. Early estimates of the indirect effects of the COVID-19 pandemic on maternal and child mortality in low-income and middle-income countries: a
modelling study. Lancet Glob Health 2020;8:e901-8.
31 Average age of those who had died with COVID-19. UK Government 2021;Jan 11.
32 Krumholz HM. Where have all the heart attacks gone? New York Times 2020;April 6.
33 Wilcock AD, Zubizarreta JR, Wadhera RK, et al. Factors underlying reduced hospitalizations for myocardial infarction during the COVID-19 pandemic. JAMA Cardiol 2024;9:914-20.
34 Ponzoni M, Morabito G, Corrao G, et al. The COVID-19 pandemic was associated with a change in therapeutic management and mortality in heart failure patients. J Clin Med 2024;13:2625.
35 Qamar A, Abramov D, Bang V, et al. Has the first year of the COVID pandemic impacted the trends in obesity-related CVD mortality between 1999 and 2019 in the United States? Int J Cardiol Cardiovasc Risk Prev 2024;21:200248.
36 Lippi G, Sanchis-Gomar F, Lavie CJ. Excess mortality for acute myocardial infarction in the United States during the first two years of the COVID-19 pandemic. Prog Cardiovasc Dis 2024;85:120-1.
37 Wai AK, Yip TF, Wong YH, et al. The Effect of the COVID-19 Pandemic on Non-COVID-19 Deaths: Population-Wide Retrospective Cohort Study. JMIR Public Health Surveill. 2024 Feb 13;10:e41792.
38 Aaby P. Malnourished or overinfected. An analysis of the determinants of acute measles
mortality. Dan Med Bull 1989;36:93-113.
39 Aaby P. Severe measles in Copenhagen, 1915–1925. Rev Infect Dis 1988;10:452-6.
40 Excess mortality during the Coronavirus pandemic (COVID-19). Our World in Data (undated).
41 COVID-19 Excess Mortality Collaborators. Estimating excess mortality due to the COVID-19 pandemic: a systematic analysis of COVID-19-related mortality, 2020-21. Lancet 2022;399:1513-36.
42 GBD 2021 Demographics Collaborators. Global age-sex-specific mortality, life expectancy, and population estimates in 204 countries and territories and 811 subnational locations, 1950-2021, and the impact of the COVID-19 pandemic: a comprehensive demographic analysis for the Global Burden of Disease Study 2021. Lancet 2024;403:1989-2056.
43 Bhattacharya J, Memoli MJ. NIH Directors: The world needs a new pandemic playbook. City Journal 2025;Nov 13.
44 NIH infectious disease researcher calls for end of dangerous virus studies. The DisInformation Chronicle 2025;May 4.



No comments:
Post a Comment